Valentino Dammassa, Francesco Corradi, Costanza Natalia Julia Colombo, Francesco Mojoli, Susanna Price, Guido Tavazzi
{"title":"Pulmonary artery acceleration time accuracy for systolic pulmonary artery pressure estimation in critically ill patients.","authors":"Valentino Dammassa, Francesco Corradi, Costanza Natalia Julia Colombo, Francesco Mojoli, Susanna Price, Guido Tavazzi","doi":"10.1186/s13089-022-00276-4","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Estimation of pulmonary pressures is of key importance in acute cardiovascular and respiratory failure. Pulmonary artery acceleration time (PAAT) has emerged as reliable parameter for the estimation of systolic pulmonary artery pressure (sPAP) in cardiological population with preserved right ventricular function. We sought to find whether PAAT correlates with sPAP in critically ill patients with and without right ventricular (RV) systolic dysfunction.</p><p><strong>Methods: </strong>Observational study. We measured sPAP using continuous-wave Doppler analysis of tricuspid regurgitation velocity peak method and we assessed the validity of PAAT in estimating sPAP in patients admitted to adult intensive care unit (ICU) for acute cardiovascular and respiratory failure.</p><p><strong>Results: </strong>We enrolled 236 patients admitted to cardiothoracic ICU for cardiovascular and respiratory failure (respectively: 129, 54.7% and 107, 45.3%). 114 (48.3%) had preserved RV systolic function (defined as TAPSE ≥ 17 mm), whilst 122 (51.7%) had RV systolic impairment (defined as TAPSE < 17 mm). A weak inverse correlation between PAAT and sPAP (ρ-0.189, p 0.0035) was observed in overall population, which was confirmed in those with preserved RV systolic PAAT and sPAP (ρ-0.361, p 0.0001). In patients with impaired RV systolic function no statistically significant correlation between PAAT and sPAP was demonstrated (p 0.2737). Adjusting PAAT values for log<sub>10</sub>, heart rate and RV ejection time did not modify the abovementioned correlations.</p><p><strong>Conclusions: </strong>PAAT measurement to derive sPAP is not reliable in cardiothoracic critically ill patients, particularly in the coexistence of RV systolic impairment.</p>","PeriodicalId":36911,"journal":{"name":"Ultrasound Journal","volume":" ","pages":"26"},"PeriodicalIF":2.9000,"publicationDate":"2022-06-20","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9209611/pdf/","citationCount":"5","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Ultrasound Journal","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1186/s13089-022-00276-4","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"Medicine","Score":null,"Total":0}
引用次数: 5
Abstract
Background: Estimation of pulmonary pressures is of key importance in acute cardiovascular and respiratory failure. Pulmonary artery acceleration time (PAAT) has emerged as reliable parameter for the estimation of systolic pulmonary artery pressure (sPAP) in cardiological population with preserved right ventricular function. We sought to find whether PAAT correlates with sPAP in critically ill patients with and without right ventricular (RV) systolic dysfunction.
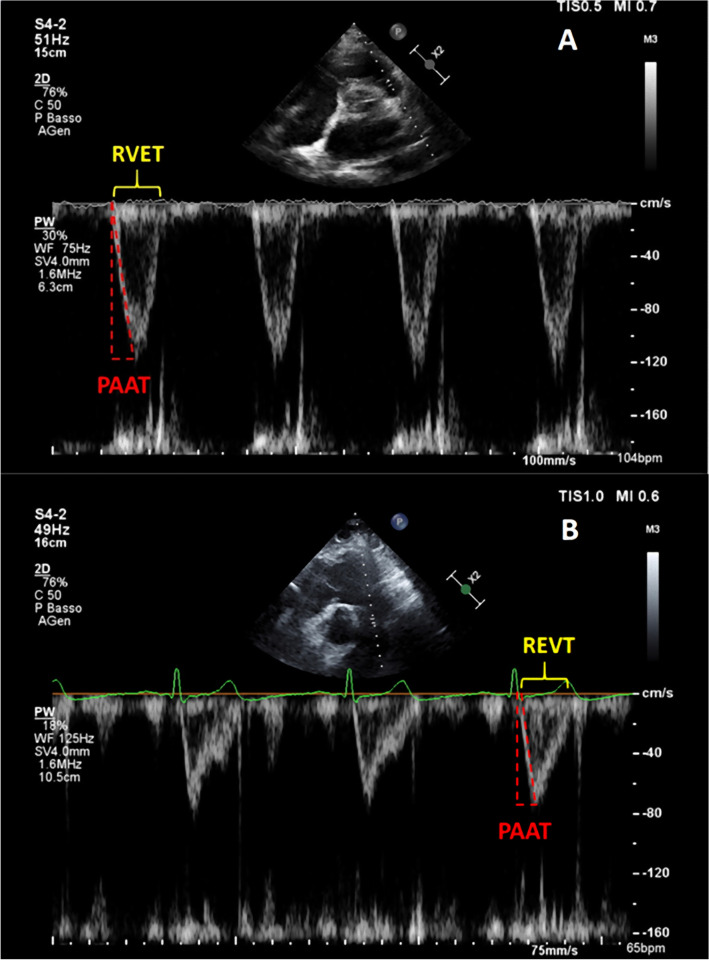
Methods: Observational study. We measured sPAP using continuous-wave Doppler analysis of tricuspid regurgitation velocity peak method and we assessed the validity of PAAT in estimating sPAP in patients admitted to adult intensive care unit (ICU) for acute cardiovascular and respiratory failure.
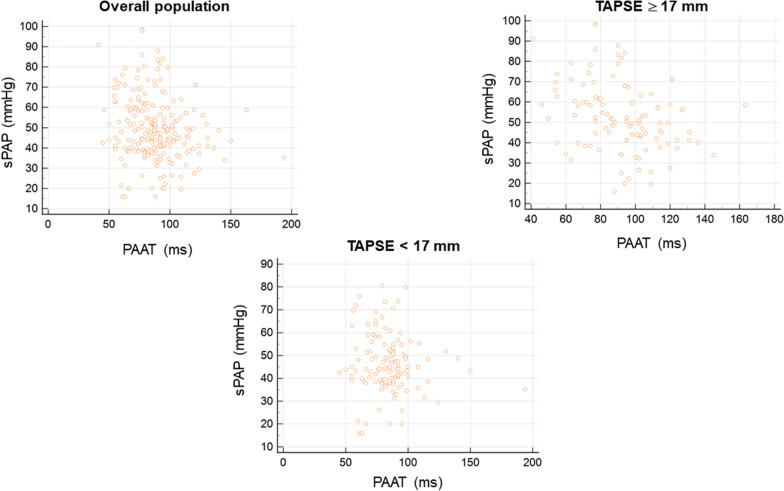
Results: We enrolled 236 patients admitted to cardiothoracic ICU for cardiovascular and respiratory failure (respectively: 129, 54.7% and 107, 45.3%). 114 (48.3%) had preserved RV systolic function (defined as TAPSE ≥ 17 mm), whilst 122 (51.7%) had RV systolic impairment (defined as TAPSE < 17 mm). A weak inverse correlation between PAAT and sPAP (ρ-0.189, p 0.0035) was observed in overall population, which was confirmed in those with preserved RV systolic PAAT and sPAP (ρ-0.361, p 0.0001). In patients with impaired RV systolic function no statistically significant correlation between PAAT and sPAP was demonstrated (p 0.2737). Adjusting PAAT values for log10, heart rate and RV ejection time did not modify the abovementioned correlations.
Conclusions: PAAT measurement to derive sPAP is not reliable in cardiothoracic critically ill patients, particularly in the coexistence of RV systolic impairment.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
