Iris Feinberg, Elizabeth L Tighe, Michelle M Ogrodnick
{"title":"Strengthening the Case for Universal Health Literacy: The Dispersion of Health Literacy Experiences Across a Southern U.S. State.","authors":"Iris Feinberg, Elizabeth L Tighe, Michelle M Ogrodnick","doi":"10.3928/24748307-20220620-01","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>How individuals perceive their health literacy may differ based on demographic and individual characteristics.</p><p><strong>Objective: </strong>The purpose of this study was to understand the dispersion of health literacy across demographics in the state of Georgia in 2021 and to determine which factors influence health literacy.</p><p><strong>Methods: </strong>Study participants were age 18 years and older and completed an on-line Health Literacy Questionnaire (<i>N</i> = 520). The participant pool was stratified to mirror state-wide demographics of geography and race. Results were further collapsed into composite scales reflecting basic, communicative, and critical health literacy. Descriptive statistics, bivariate Pearson's correlations, and multiple regression analyses were used. A two-step cluster analysis was performed with the nine health literacy scales.</p><p><strong>Key results: </strong>Rural county and no health insurance were negatively related to all three composite scales (<i>rs</i> = .093-.254, <i>ps</i> < .05). Demographic predictors accounted for 6.7% of the variance in basic (F[6, 439] = 5.287, <i>p</i> < .001), 10% in communicative (F[6, 438] = 8.154, <i>p</i> < .001), and 6% for critical (F[6, 439] = 4.675, <i>p</i> < .0010. In all scales, health insurance status was the strongest primary unique predictor (<i>βs</i> = .236, .295, .181, ps <.05, respectively). In a two-step cluster analysis only health insurance status differentiated the health literacy level clusters (<i>X</i><sup>2</sup>(3) = 9.43, 34.51, <i>ps</i> = 024, <.001 respectively).</p><p><strong>Conclusion: </strong>Lacking health insurance is the most consistent and largest contributor to low health literacy across the state of Georgia; population demographics are not. Health literacy policies and practices should be developed for universal application and not focus on specific populations. [<b><i>HLRP: Health Literacy Research and Practice</i>. 2022;6(3):e182-e190.</b>] Plain Language Summary: In this study, demographics that are usually associated with low health literacy like age, sex, race, educational attainment, and type of county (rural or urban) were not associated with; the only significant factor was lack of health insurance. This relationship strengthens the case for universal health literacy precautions that go beyond population demographics.</p>","PeriodicalId":36651,"journal":{"name":"Health literacy research and practice","volume":" ","pages":"e182-e190"},"PeriodicalIF":0.0000,"publicationDate":"2022-07-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9272571/pdf/","citationCount":"1","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Health literacy research and practice","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.3928/24748307-20220620-01","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2022/7/8 0:00:00","PubModel":"Epub","JCR":"Q2","JCRName":"Medicine","Score":null,"Total":0}
引用次数: 1
Abstract
Background: How individuals perceive their health literacy may differ based on demographic and individual characteristics.
Objective: The purpose of this study was to understand the dispersion of health literacy across demographics in the state of Georgia in 2021 and to determine which factors influence health literacy.
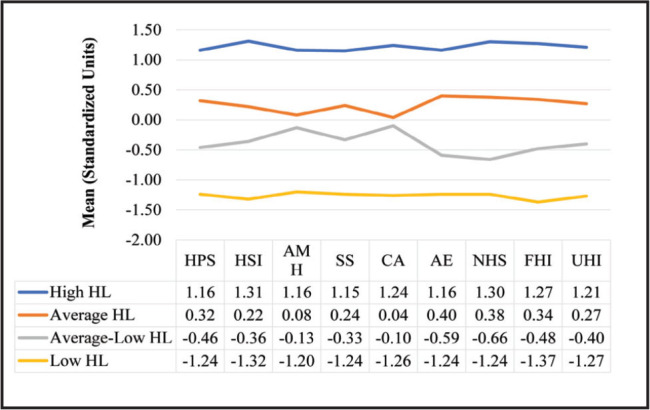
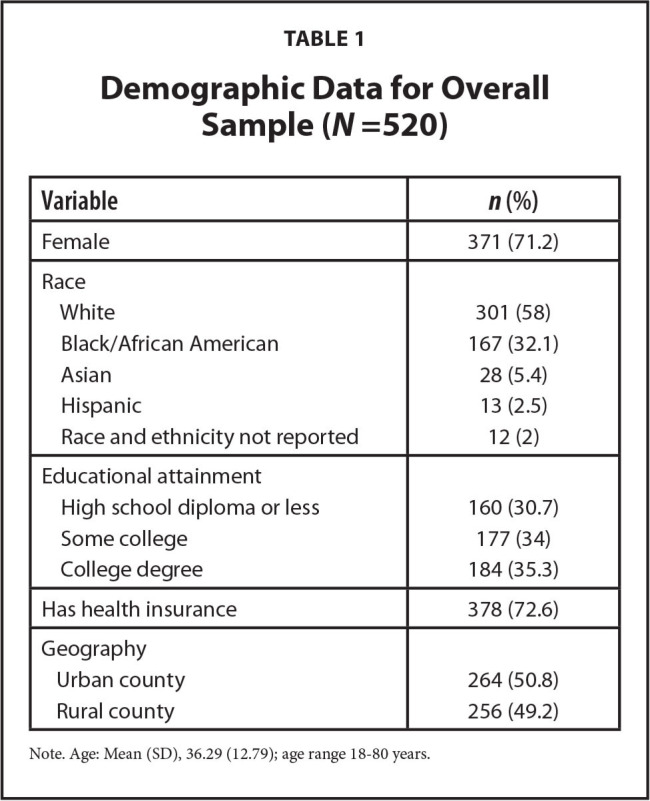
Methods: Study participants were age 18 years and older and completed an on-line Health Literacy Questionnaire (N = 520). The participant pool was stratified to mirror state-wide demographics of geography and race. Results were further collapsed into composite scales reflecting basic, communicative, and critical health literacy. Descriptive statistics, bivariate Pearson's correlations, and multiple regression analyses were used. A two-step cluster analysis was performed with the nine health literacy scales.
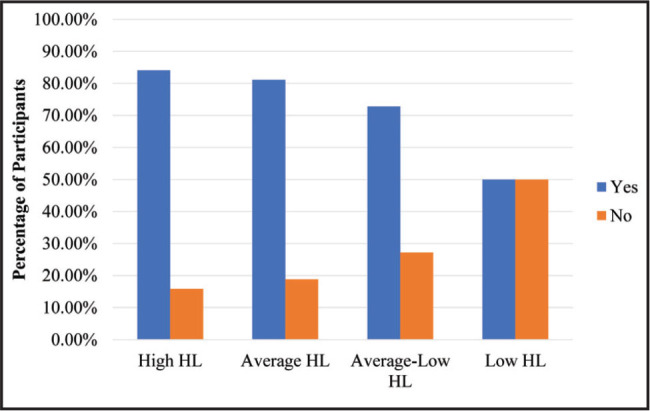
Key results: Rural county and no health insurance were negatively related to all three composite scales (rs = .093-.254, ps < .05). Demographic predictors accounted for 6.7% of the variance in basic (F[6, 439] = 5.287, p < .001), 10% in communicative (F[6, 438] = 8.154, p < .001), and 6% for critical (F[6, 439] = 4.675, p < .0010. In all scales, health insurance status was the strongest primary unique predictor (βs = .236, .295, .181, ps <.05, respectively). In a two-step cluster analysis only health insurance status differentiated the health literacy level clusters (X2(3) = 9.43, 34.51, ps = 024, <.001 respectively).
Conclusion: Lacking health insurance is the most consistent and largest contributor to low health literacy across the state of Georgia; population demographics are not. Health literacy policies and practices should be developed for universal application and not focus on specific populations. [HLRP: Health Literacy Research and Practice. 2022;6(3):e182-e190.] Plain Language Summary: In this study, demographics that are usually associated with low health literacy like age, sex, race, educational attainment, and type of county (rural or urban) were not associated with; the only significant factor was lack of health insurance. This relationship strengthens the case for universal health literacy precautions that go beyond population demographics.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
