{"title":"The Diagnostic Challenge of Sialolithiasis.","authors":"Sahar M N Bukhary","doi":"10.4103/jmau.jmau_92_22","DOIUrl":null,"url":null,"abstract":"<p><p>The major salivary glands (parotid, submandibular, and sublingual) are most frequently obstructed by calculi within the salivary gland, or more uncommonly, by ranulas. Despite the well-defined clinical and radiographic diagnostic features, sialolithiasis may sometimes be confused with sialadenitis and ranulas, especially when encountered in general dental practice. We, therefore, present a case that illustrates this diagnostic dilemma to highlight the salient features of all three conditions. A 28-year-old female presented with a history of a submandibular swelling for 8 months. On intraoral examination, a bluish sublingual swelling was identified at the left side of the lingual frenum, causing a slight elevation of the tongue. The preliminary diagnosis was of a ranula; however, the clinical history suggested sialolithiasis. A hard structure was palpated in the submandibular gland, and a mandibular occlusal film revealed a large ductal sialolith. Sialolithotomy was performed under local anesthesia, and a single 7.2 mm stone was retrieved. The postoperative follow-up period was uneventful, with good healing and restored normal salivary flow. Despite the fairly clear clinical and radiographic diagnostic criteria suggestive of sialolithiasis, the bluish-tinged swelling of the floor of the mouth prompted the examining dentist to provisionally diagnose a ranula. Sialolithiasis is a common obstructive condition of the salivary gland encountered in the dental setting. Despite the clinical and radiographic features usually guiding the correct diagnosis, it can be a challenging diagnosis for less experienced dentists, who must always carefully consider the history, clinical, and radiographic findings.</p>","PeriodicalId":16340,"journal":{"name":"Journal of Microscopy and Ultrastructure","volume":"1 1","pages":"221-224"},"PeriodicalIF":0.0000,"publicationDate":"2023-02-07","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11729025/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Microscopy and Ultrastructure","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.4103/jmau.jmau_92_22","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/10/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"Medicine","Score":null,"Total":0}
引用次数: 0
Abstract
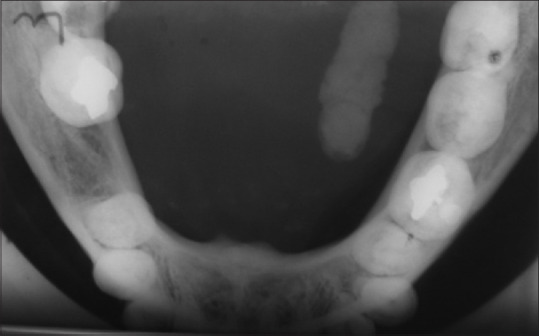
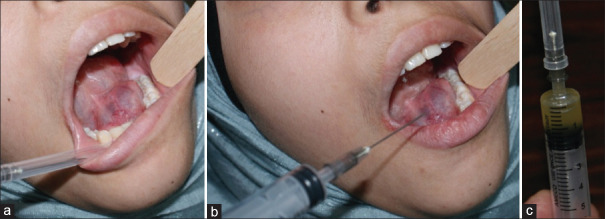
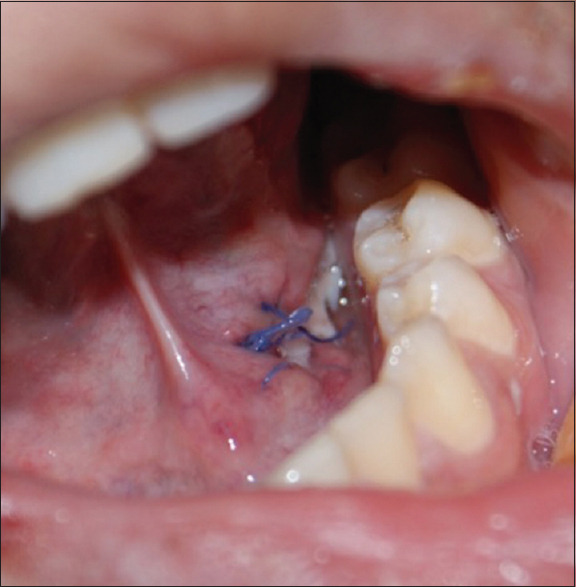
The major salivary glands (parotid, submandibular, and sublingual) are most frequently obstructed by calculi within the salivary gland, or more uncommonly, by ranulas. Despite the well-defined clinical and radiographic diagnostic features, sialolithiasis may sometimes be confused with sialadenitis and ranulas, especially when encountered in general dental practice. We, therefore, present a case that illustrates this diagnostic dilemma to highlight the salient features of all three conditions. A 28-year-old female presented with a history of a submandibular swelling for 8 months. On intraoral examination, a bluish sublingual swelling was identified at the left side of the lingual frenum, causing a slight elevation of the tongue. The preliminary diagnosis was of a ranula; however, the clinical history suggested sialolithiasis. A hard structure was palpated in the submandibular gland, and a mandibular occlusal film revealed a large ductal sialolith. Sialolithotomy was performed under local anesthesia, and a single 7.2 mm stone was retrieved. The postoperative follow-up period was uneventful, with good healing and restored normal salivary flow. Despite the fairly clear clinical and radiographic diagnostic criteria suggestive of sialolithiasis, the bluish-tinged swelling of the floor of the mouth prompted the examining dentist to provisionally diagnose a ranula. Sialolithiasis is a common obstructive condition of the salivary gland encountered in the dental setting. Despite the clinical and radiographic features usually guiding the correct diagnosis, it can be a challenging diagnosis for less experienced dentists, who must always carefully consider the history, clinical, and radiographic findings.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
