Husam A Almajali, Ali M Abu Dalo, Nidal M Al-Soud, Ali Almajali, Abdelrazzaq Alrfooh, Thani Alawamreh, Hamza Al-Wreikat
{"title":"Intramuscular Ketamine Effect on Postnasal Surgery Agitation: A Prospective Double-Blinded Randomized Controlled Trial.","authors":"Husam A Almajali, Ali M Abu Dalo, Nidal M Al-Soud, Ali Almajali, Abdelrazzaq Alrfooh, Thani Alawamreh, Hamza Al-Wreikat","doi":"10.1155/2023/2286451","DOIUrl":null,"url":null,"abstract":"<p><p>This study investigates the effect of intramuscular ketamine on emergence agitation (EA) following septoplasty and open septorhinoplasty (OSRP) when administered at subanesthetic doses at the end of surgery. A random sample of 160 ASA I-II adult patients who underwent septoplasty or OSRP between May and October, 2022, was divided into two groups of eighty patients each: ketamine (Group K) and saline (Group S) with the latter serving as the control group. At the end of surgery immediately after turning off the inhalational agent, Group K was administered with intramuscular 2 ml of normal saline containing 0.7 mg/kg ketamine and Group S with 2 ml of intramuscular normal saline. Sedation and agitation scores at emergence from anesthesia were recorded after extubation using the Richmond Agitation-Sedation Scale (RASS). The incidence of EA was higher in the saline group than in the ketamine group (56.3% vs. 5%; odds ratio (OR): 0.033; 95% confidence interval (CI): 0.010-0.103; <i>p</i> < 0.001). Variables associated with a higher incidence of agitation were ASA II classification (OR: 3.286; 95% (CI): 1.359-7.944; <i>p</i>=0.008), longer duration of surgery (OR: 1.010; 95% CI: 1.001-1.020; <i>p</i>=0.031), and OSRP surgery (OR: 2.157; CI: 1.056-5.999; <i>p</i>=0.037). The study concluded that the administration of intramuscular ketamine at a dose of 0.7 mg/kg at the end of surgery effectively reduced the incidence of EA in septoplasty and OSRP surgery.</p>","PeriodicalId":7834,"journal":{"name":"Anesthesiology Research and Practice","volume":"2023 ","pages":"2286451"},"PeriodicalIF":1.3000,"publicationDate":"2023-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9988369/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Anesthesiology Research and Practice","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1155/2023/2286451","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"ANESTHESIOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
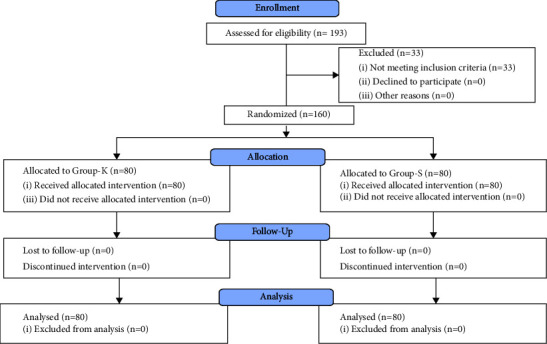
This study investigates the effect of intramuscular ketamine on emergence agitation (EA) following septoplasty and open septorhinoplasty (OSRP) when administered at subanesthetic doses at the end of surgery. A random sample of 160 ASA I-II adult patients who underwent septoplasty or OSRP between May and October, 2022, was divided into two groups of eighty patients each: ketamine (Group K) and saline (Group S) with the latter serving as the control group. At the end of surgery immediately after turning off the inhalational agent, Group K was administered with intramuscular 2 ml of normal saline containing 0.7 mg/kg ketamine and Group S with 2 ml of intramuscular normal saline. Sedation and agitation scores at emergence from anesthesia were recorded after extubation using the Richmond Agitation-Sedation Scale (RASS). The incidence of EA was higher in the saline group than in the ketamine group (56.3% vs. 5%; odds ratio (OR): 0.033; 95% confidence interval (CI): 0.010-0.103; p < 0.001). Variables associated with a higher incidence of agitation were ASA II classification (OR: 3.286; 95% (CI): 1.359-7.944; p=0.008), longer duration of surgery (OR: 1.010; 95% CI: 1.001-1.020; p=0.031), and OSRP surgery (OR: 2.157; CI: 1.056-5.999; p=0.037). The study concluded that the administration of intramuscular ketamine at a dose of 0.7 mg/kg at the end of surgery effectively reduced the incidence of EA in septoplasty and OSRP surgery.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
