{"title":"Hormone Therapy with or without Platelet-Rich Plasma (PRP) for Treatment Asherman Syndrome; A Randomized Clinical Trial.","authors":"Elham Naghshineh, Safoura Rouholamin, Zahra Derakhshandeh","doi":"10.4103/abr.abr_411_21","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Asherman syndrome is a controversial issue in obstetrics and gynecology without any consensus on its management and treatment. It is characterized by variable lesions inside the uterine cavity and also causes menstrual irregularities, infertility, and placental abnormalities. The study aimed to assess the platelet-rich plasma (PRP) effect in women with intrauterine adhesions by evaluating the improvement of the menstrual cycle and intrauterine adhesion (IUA) stage.</p><p><strong>Materials and methods: </strong>This clinical trial study was performed on 60 women with Asherman syndrome in two groups of 30. For the first group, only hormone therapy was performed and for the second group, hormone therapy with platelet-rich plasma after hysteroscopy. Recovery of Asherman syndrome and IUA stage was assessed at 6 to 8 weeks after hysteroscopy and compared between the two groups.</p><p><strong>Results: </strong>Our results demonstrated that there was no significant difference between demographic data in the two groups as well as the menstrual pattern of both groups before or after treatment (<i>P</i> > 0.05). Frequency distribution of IUA after the intervention in the PRP + hormone therapy group in grade I, II, and III were equal to 73.3%, 20%, and 6.7% and in the hormone therapy group were 53.3%, 26.7%, and 20%, respectively (<i>P</i> = 0.22). In addition, hypo menorrhea was observed in 33.3% of PRP + hormone therapy group and 40% of the hormone therapy group with no significant difference between the two groups (<i>P</i> = 0.71).</p><p><strong>Conclusion: </strong>Hormone therapy with PRP compared to hormone therapy alone after routine surgical treatment had not a significant effect on the IUA stage, duration, and severity of menstruation.</p>","PeriodicalId":7225,"journal":{"name":"Advanced Biomedical Research","volume":"12 ","pages":"17"},"PeriodicalIF":0.0000,"publicationDate":"2023-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/54/75/ABR-12-17.PMC10012034.pdf","citationCount":"3","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Advanced Biomedical Research","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.4103/abr.abr_411_21","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 3
Abstract
Background: Asherman syndrome is a controversial issue in obstetrics and gynecology without any consensus on its management and treatment. It is characterized by variable lesions inside the uterine cavity and also causes menstrual irregularities, infertility, and placental abnormalities. The study aimed to assess the platelet-rich plasma (PRP) effect in women with intrauterine adhesions by evaluating the improvement of the menstrual cycle and intrauterine adhesion (IUA) stage.
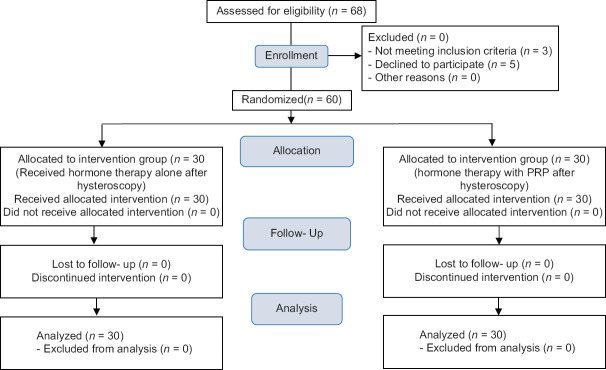
Materials and methods: This clinical trial study was performed on 60 women with Asherman syndrome in two groups of 30. For the first group, only hormone therapy was performed and for the second group, hormone therapy with platelet-rich plasma after hysteroscopy. Recovery of Asherman syndrome and IUA stage was assessed at 6 to 8 weeks after hysteroscopy and compared between the two groups.
Results: Our results demonstrated that there was no significant difference between demographic data in the two groups as well as the menstrual pattern of both groups before or after treatment (P > 0.05). Frequency distribution of IUA after the intervention in the PRP + hormone therapy group in grade I, II, and III were equal to 73.3%, 20%, and 6.7% and in the hormone therapy group were 53.3%, 26.7%, and 20%, respectively (P = 0.22). In addition, hypo menorrhea was observed in 33.3% of PRP + hormone therapy group and 40% of the hormone therapy group with no significant difference between the two groups (P = 0.71).
Conclusion: Hormone therapy with PRP compared to hormone therapy alone after routine surgical treatment had not a significant effect on the IUA stage, duration, and severity of menstruation.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
