Jonas Auer, Joachim Braun, Julian Lenk, Johannes Gollrad, Sa-Ra Ro, Bernd Hamm, Maximilian de Bucourt
{"title":"Tunneled hemodialysis catheter insertion: Above, within, or below the right atrium-Where is the tip?","authors":"Jonas Auer, Joachim Braun, Julian Lenk, Johannes Gollrad, Sa-Ra Ro, Bernd Hamm, Maximilian de Bucourt","doi":"10.1177/20584601221122421","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>One major challenge when inserting a tunneled, cuffed central venous catheter (CVC) for hemodialysis under fluoroscopy is to accurately place the catheter tip by assessing its position in relation to the cardiac silhouette to approximate the right atrium (RA).</p><p><strong>Purpose: </strong>To investigate whether a weighted mean calculated from published results for two two-dimensional landmark reference distances may be useful in assessing CVC tip positions in relation to the RA.</p><p><strong>Material and methods: </strong>Central venous catheter tip positions attained under fluoroscopic imaging during insertion using the cardiac silhouette as approximation were retrospectively related to two reference distances (carina to cranial RA border and craniocaudal RA extent), which were used to group catheter tip locations above (1), within (2), or below (3) the RA (henceforth referred to as landmark technique approximation, LTA). The LTA-derived catheter tip locations were validated by correlation with postinterventional computed tomography (CT) datasets acquired shortly after implantation (if available).</p><p><strong>Results: </strong>Based on LTA, 45 catheter tips (10.6%) were above, 179 (42.2%) within, and 200 (47.2%) below the RA. Postinterventional CT (<i>n</i> = 57; 13.4%) visualized 26.3% above, 66.7% within, and 7.0% below the RA.</p><p><strong>Conclusion: </strong>The LTA reference distances appear to lead to a rather low categorization of the CVC tips, or the tips have been placed rather low in the study population. Validation using postinterventional CT indicated an underestimation of the RA in the LTA. Patient characteristics with a higher risk of false estimation through LTA have been defined.</p>","PeriodicalId":72063,"journal":{"name":"Acta radiologica open","volume":"11 9","pages":"20584601221122421"},"PeriodicalIF":1.0000,"publicationDate":"2022-09-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/a5/bd/10.1177_20584601221122421.PMC9483979.pdf","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Acta radiologica open","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1177/20584601221122421","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q4","JCRName":"RADIOLOGY, NUCLEAR MEDICINE & MEDICAL IMAGING","Score":null,"Total":0}
引用次数: 0
Abstract
Background: One major challenge when inserting a tunneled, cuffed central venous catheter (CVC) for hemodialysis under fluoroscopy is to accurately place the catheter tip by assessing its position in relation to the cardiac silhouette to approximate the right atrium (RA).
Purpose: To investigate whether a weighted mean calculated from published results for two two-dimensional landmark reference distances may be useful in assessing CVC tip positions in relation to the RA.
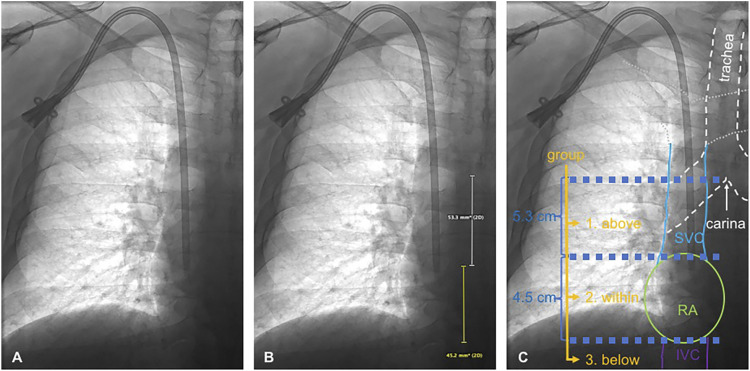
Material and methods: Central venous catheter tip positions attained under fluoroscopic imaging during insertion using the cardiac silhouette as approximation were retrospectively related to two reference distances (carina to cranial RA border and craniocaudal RA extent), which were used to group catheter tip locations above (1), within (2), or below (3) the RA (henceforth referred to as landmark technique approximation, LTA). The LTA-derived catheter tip locations were validated by correlation with postinterventional computed tomography (CT) datasets acquired shortly after implantation (if available).
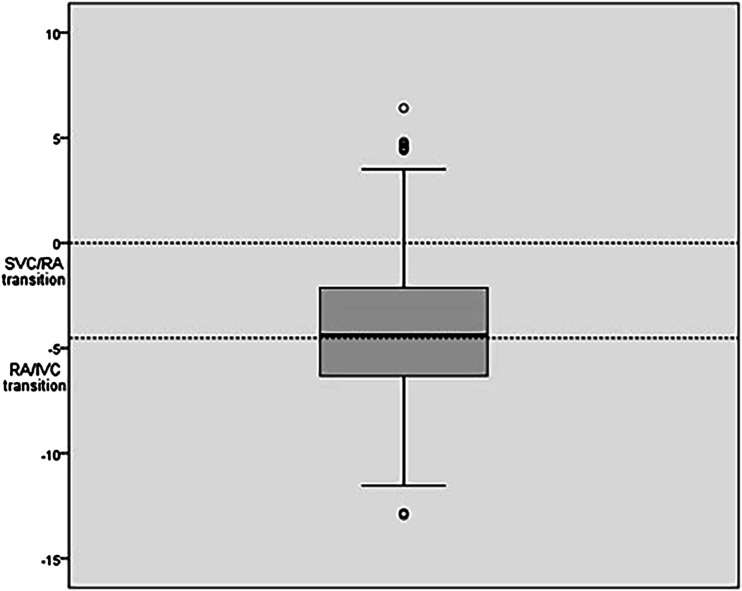
Results: Based on LTA, 45 catheter tips (10.6%) were above, 179 (42.2%) within, and 200 (47.2%) below the RA. Postinterventional CT (n = 57; 13.4%) visualized 26.3% above, 66.7% within, and 7.0% below the RA.
Conclusion: The LTA reference distances appear to lead to a rather low categorization of the CVC tips, or the tips have been placed rather low in the study population. Validation using postinterventional CT indicated an underestimation of the RA in the LTA. Patient characteristics with a higher risk of false estimation through LTA have been defined.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
