{"title":"The Use of Putative Dialysis Initiation Time in Comparative Outcomes of Patients with Advanced Chronic Kidney Disease: Methodological Aspects.","authors":"Danh V Nguyen, Esra Kurum, Damla Senturk","doi":"10.6000/1929-6029.2022.11.16","DOIUrl":null,"url":null,"abstract":"<p><p>The latest data from the United States Renal Data Systems show over 134,000 individuals with end-stage kidney disease (ESKD) starting dialysis in the year 2019. ESKD patients on dialysis, the default treatment strategy, have high mortality and hospitalization, especially in the first year of dialysis. An alternative treatment strategy is (non-dialysis) conservative management (CM). The relative effectiveness of CM with respect to various patient outcomes, including survival, hospitalization, and health-related quality of life among others, especially in elderly ESKD or advanced chronic kidney disease patients with serious comorbidities, is an active area of research. A technical challenge inherent in comparing patient outcomes between CM and dialysis patient groups is that the start of follow-up time is \"not defined\" for patients on CM because they do not initiate dialysis. One solution is the use of putative dialysis initiation (PDI) time. In this work, we examine the validity of the use of PDI time to determine the start of follow-up for longitudinal retrospective and prospective cohort studies involving CM. We propose and assess the efficacy of estimating PDI time using linear mixed effects model of kidney function decline over time via simulation studies. We also illustrate how the estimated PDI time can be used to effectively estimate the survival distribution.</p>","PeriodicalId":73480,"journal":{"name":"International journal of statistics in medical research","volume":"11 ","pages":"128-135"},"PeriodicalIF":0.0000,"publicationDate":"2022-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10241465/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"International journal of statistics in medical research","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.6000/1929-6029.2022.11.16","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
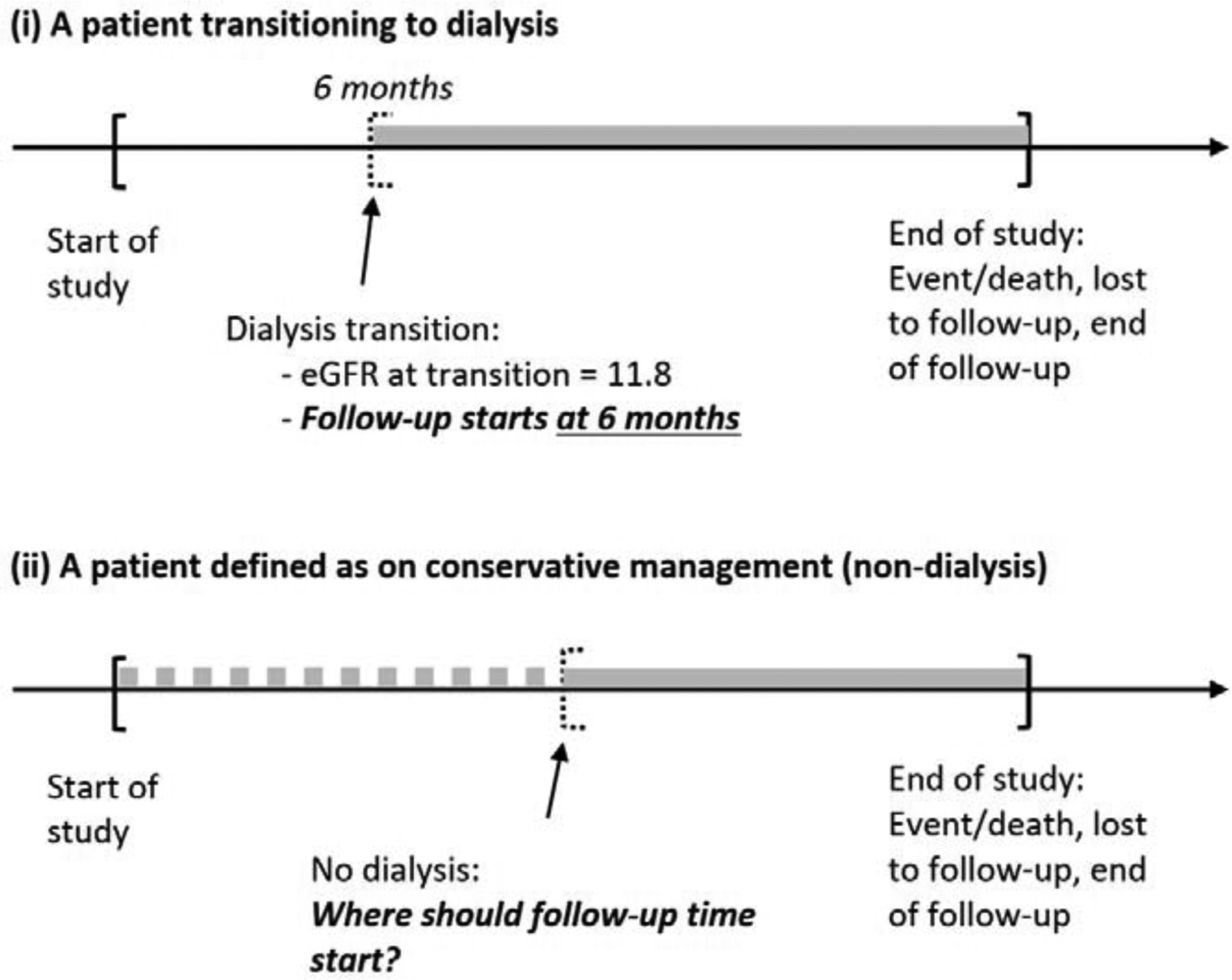
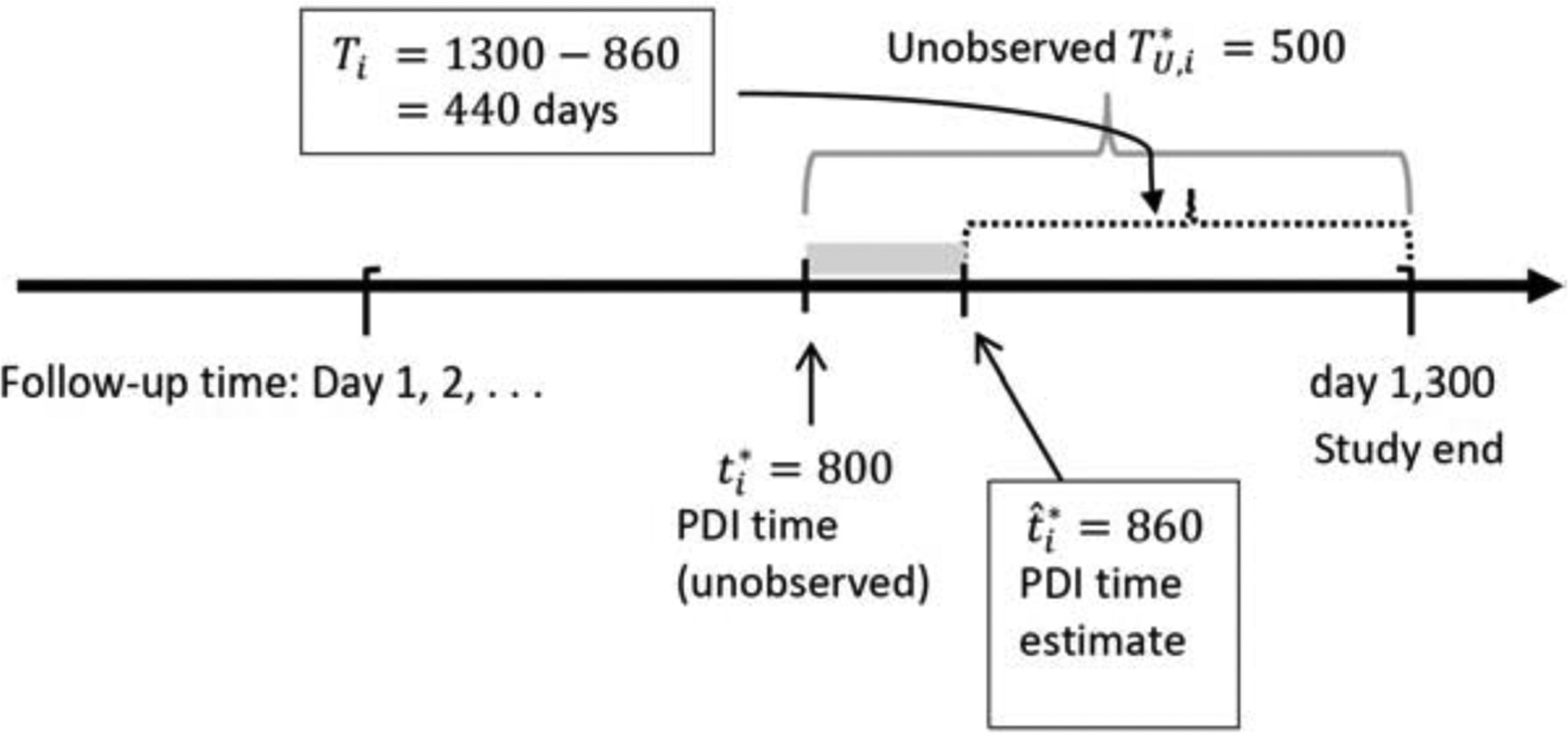
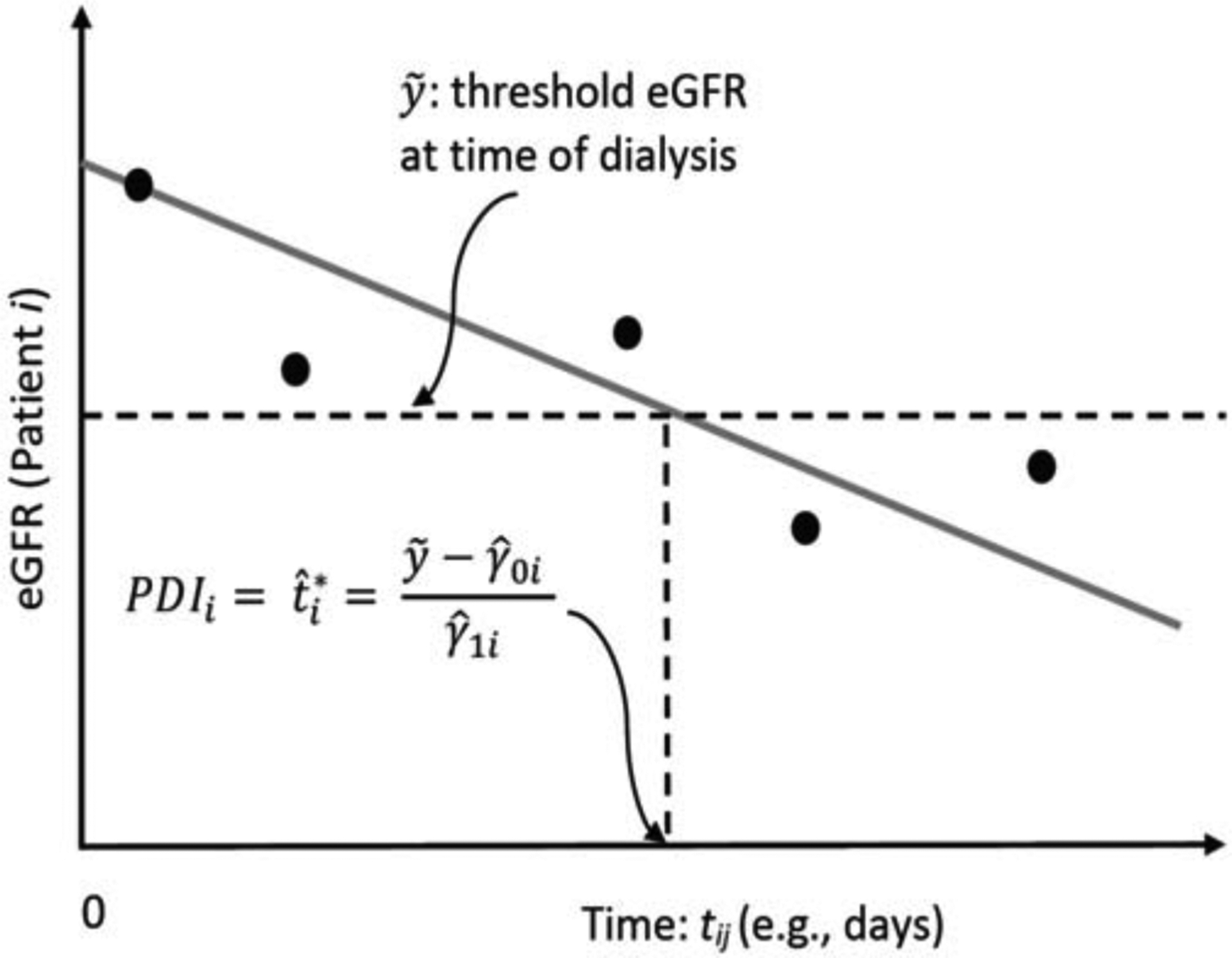
The latest data from the United States Renal Data Systems show over 134,000 individuals with end-stage kidney disease (ESKD) starting dialysis in the year 2019. ESKD patients on dialysis, the default treatment strategy, have high mortality and hospitalization, especially in the first year of dialysis. An alternative treatment strategy is (non-dialysis) conservative management (CM). The relative effectiveness of CM with respect to various patient outcomes, including survival, hospitalization, and health-related quality of life among others, especially in elderly ESKD or advanced chronic kidney disease patients with serious comorbidities, is an active area of research. A technical challenge inherent in comparing patient outcomes between CM and dialysis patient groups is that the start of follow-up time is "not defined" for patients on CM because they do not initiate dialysis. One solution is the use of putative dialysis initiation (PDI) time. In this work, we examine the validity of the use of PDI time to determine the start of follow-up for longitudinal retrospective and prospective cohort studies involving CM. We propose and assess the efficacy of estimating PDI time using linear mixed effects model of kidney function decline over time via simulation studies. We also illustrate how the estimated PDI time can be used to effectively estimate the survival distribution.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
