Efficacy and Safety of Abrocitinib in Patients with Severe and/or Difficult-to-Treat Atopic Dermatitis: A Post Hoc Analysis of the Randomized Phase 3 JADE COMPARE Trial
Eric L. Simpson, Jonathan I. Silverberg, Jacob P. Thyssen, Manuelle Viguier, Diamant Thaçi, Marjolein de Bruin-Weller, Stephan Weidinger, Gary Chan, Marco DiBonaventura, Pinaki Biswas, Claire Feeney, Christopher Koulias, Michael J. Cork
{"title":"Efficacy and Safety of Abrocitinib in Patients with Severe and/or Difficult-to-Treat Atopic Dermatitis: A Post Hoc Analysis of the Randomized Phase 3 JADE COMPARE Trial","authors":"Eric L. Simpson, Jonathan I. Silverberg, Jacob P. Thyssen, Manuelle Viguier, Diamant Thaçi, Marjolein de Bruin-Weller, Stephan Weidinger, Gary Chan, Marco DiBonaventura, Pinaki Biswas, Claire Feeney, Christopher Koulias, Michael J. Cork","doi":"10.1007/s40257-023-00785-5","DOIUrl":null,"url":null,"abstract":"<div><h3>Background</h3><p>Traditional systemic immunosuppressants and advanced therapies improve signs and symptoms of moderate-to-severe atopic dermatitis (AD). However, data are limited in severe and/or difficult-to-treat AD. In the phase 3 JADE COMPARE trial of patients with moderate-to-severe AD receiving background topical therapy, once-daily abrocitinib 200 mg and 100 mg showed significantly greater reductions in the symptoms of AD than placebo and significantly greater improvement in itch response (with abrocitinib 200 mg) than dupilumab at week 2.</p><h3>Objective</h3><p>This study assessed the efficacy and safety of abrocitinib and dupilumab in a subset of patients with severe and/or difficult-to-treat AD in a post hoc analysis of the JADE COMPARE trial.</p><h3>Methods</h3><p>Adults with moderate-to-severe AD received once-daily oral abrocitinib 200 mg or 100 mg, dupilumab 300 mg subcutaneous injection every 2 weeks, or placebo with concomitant medicated topical therapy. Severe and/or difficult-to-treat AD subgroups were classified by baseline characteristics [Investigator’s Global Assessment (IGA) 4, Eczema Area and Severity Index (EASI) > 21, failure or intolerance to prior systemic agents (excluding patients who took only corticosteroids), percentage of body surface area (%BSA) > 50, upper quartiles of EASI (EASI > 38) and %BSA (%BSA > 65), and combined subgroup of IGA 4, EASI > 21, and %BSA > 50, and failure or intolerance to prior systemic agents (excluding patients who took only corticosteroids)]. Assessments included IGA score of 0 (clear) or 1 (almost clear) and a ≥ 2-point improvement from baseline, ≥ 75% and ≥ 90% improvement from baseline in EASI (EASI-75 and EASI-90), ≥ 4-point improvement from baseline in Peak Pruritus-Numerical Rating Scale (PP-NRS4), time to PP-NRS4, least squares mean (LSM) change from baseline in 14-day PP-NRS (days 2–15), Patient-Oriented Eczema Measure (POEM), and Dermatology Life Quality Index (DLQI) up to week 16.</p><h3>Results</h3><p>The proportion of patients achieving IGA 0/1, EASI-75, and EASI-90 responses was significantly greater with abrocitinib 200 mg than placebo (nominal <i>p</i> < 0.05) across all subgroups with severe and/or difficult-to-treat AD. Across most subgroups, PP-NRS4 response was significantly greater with abrocitinib 200 mg than placebo (nominal <i>p</i> < 0.01); the time to achieve this response was shorter with abrocitinib 200 mg (range 4.5–6.0 days) than abrocitinib 100 mg (range 5.0–17.0 days), dupilumab (range 8.0–11.0 days), and placebo (range 3.0–11.5 days). LSM change from baseline in POEM and DLQI was significantly greater with abrocitinib 200 mg than placebo (nominal <i>p</i> < 0.001) across all subgroups. Clinically meaningful differences were observed between abrocitinib and dupilumab for most evaluated endpoints across several subgroups, including in patients who failed or were intolerant to prior systemic therapy.</p><h3>Conclusions</h3><p>Abrocitinib provided rapid and substantially greater improvements in skin clearance and quality of life compared with placebo and dupilumab in subgroups of patients with severe and/or difficult-to-treat AD. These findings support the use of abrocitinib for severe and/or difficult-to-treat AD.</p><h3>Trial registration:</h3><p>ClinicalTrials.gov, NCT03720470.</p></div>","PeriodicalId":7706,"journal":{"name":"American Journal of Clinical Dermatology","volume":"24 4","pages":"609 - 621"},"PeriodicalIF":8.8000,"publicationDate":"2023-05-22","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/cd/95/40257_2023_Article_785.PMC10293387.pdf","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"American Journal of Clinical Dermatology","FirstCategoryId":"3","ListUrlMain":"https://link.springer.com/article/10.1007/s40257-023-00785-5","RegionNum":1,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"DERMATOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Background
Traditional systemic immunosuppressants and advanced therapies improve signs and symptoms of moderate-to-severe atopic dermatitis (AD). However, data are limited in severe and/or difficult-to-treat AD. In the phase 3 JADE COMPARE trial of patients with moderate-to-severe AD receiving background topical therapy, once-daily abrocitinib 200 mg and 100 mg showed significantly greater reductions in the symptoms of AD than placebo and significantly greater improvement in itch response (with abrocitinib 200 mg) than dupilumab at week 2.
Objective
This study assessed the efficacy and safety of abrocitinib and dupilumab in a subset of patients with severe and/or difficult-to-treat AD in a post hoc analysis of the JADE COMPARE trial.
Methods
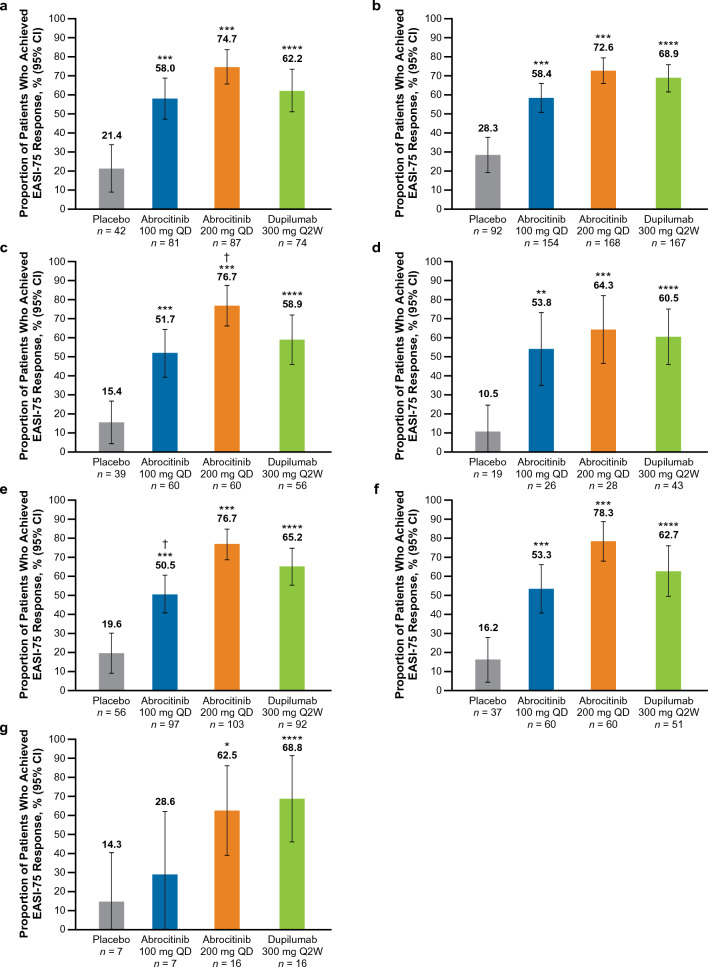
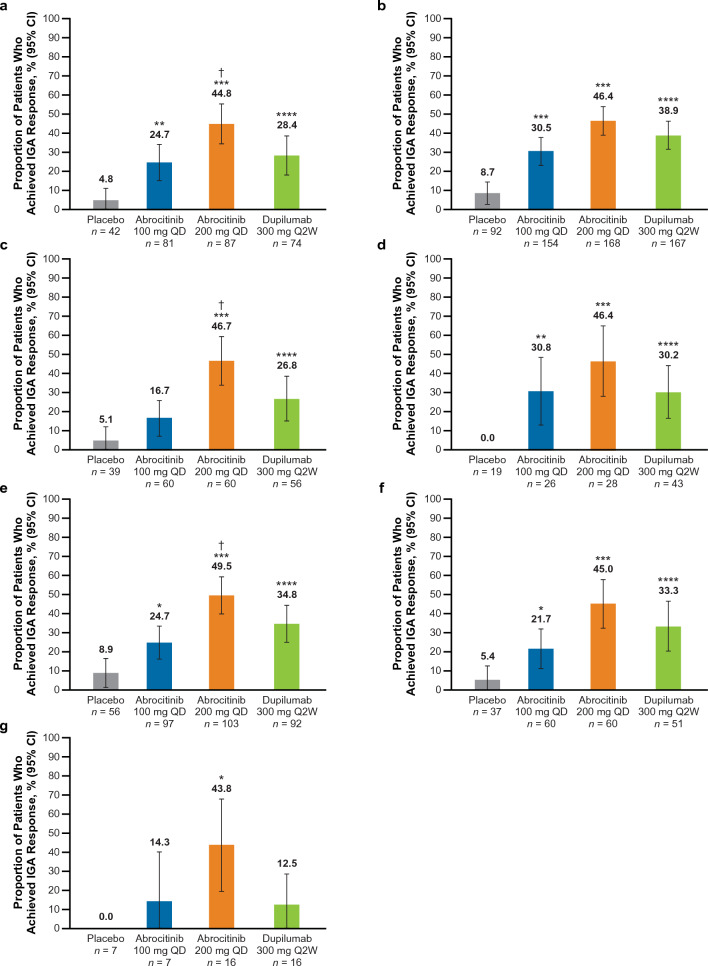
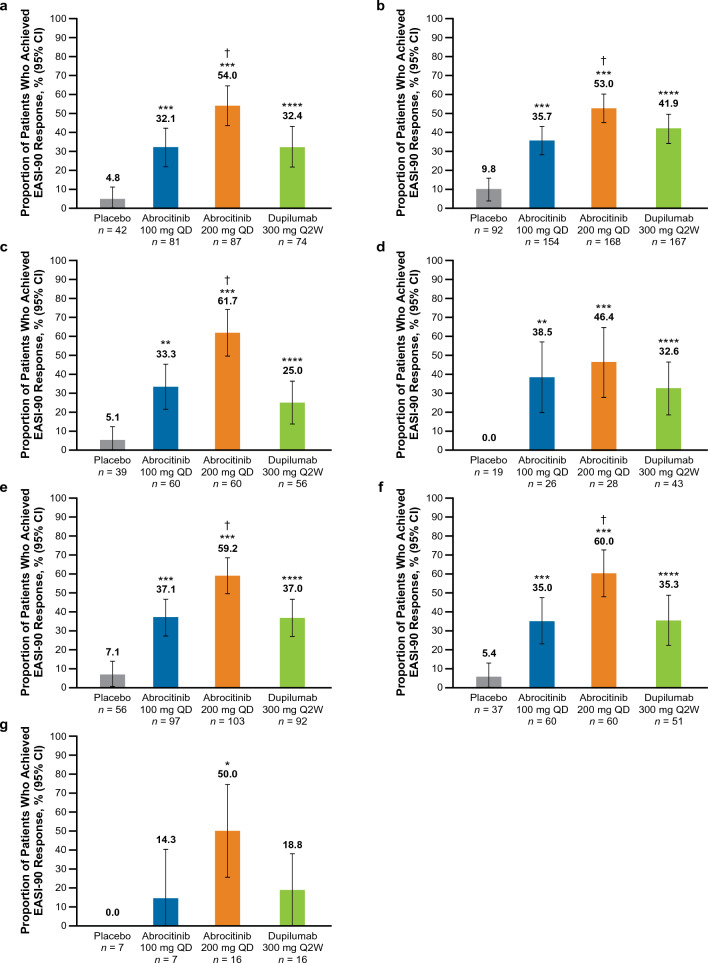
Adults with moderate-to-severe AD received once-daily oral abrocitinib 200 mg or 100 mg, dupilumab 300 mg subcutaneous injection every 2 weeks, or placebo with concomitant medicated topical therapy. Severe and/or difficult-to-treat AD subgroups were classified by baseline characteristics [Investigator’s Global Assessment (IGA) 4, Eczema Area and Severity Index (EASI) > 21, failure or intolerance to prior systemic agents (excluding patients who took only corticosteroids), percentage of body surface area (%BSA) > 50, upper quartiles of EASI (EASI > 38) and %BSA (%BSA > 65), and combined subgroup of IGA 4, EASI > 21, and %BSA > 50, and failure or intolerance to prior systemic agents (excluding patients who took only corticosteroids)]. Assessments included IGA score of 0 (clear) or 1 (almost clear) and a ≥ 2-point improvement from baseline, ≥ 75% and ≥ 90% improvement from baseline in EASI (EASI-75 and EASI-90), ≥ 4-point improvement from baseline in Peak Pruritus-Numerical Rating Scale (PP-NRS4), time to PP-NRS4, least squares mean (LSM) change from baseline in 14-day PP-NRS (days 2–15), Patient-Oriented Eczema Measure (POEM), and Dermatology Life Quality Index (DLQI) up to week 16.
Results
The proportion of patients achieving IGA 0/1, EASI-75, and EASI-90 responses was significantly greater with abrocitinib 200 mg than placebo (nominal p < 0.05) across all subgroups with severe and/or difficult-to-treat AD. Across most subgroups, PP-NRS4 response was significantly greater with abrocitinib 200 mg than placebo (nominal p < 0.01); the time to achieve this response was shorter with abrocitinib 200 mg (range 4.5–6.0 days) than abrocitinib 100 mg (range 5.0–17.0 days), dupilumab (range 8.0–11.0 days), and placebo (range 3.0–11.5 days). LSM change from baseline in POEM and DLQI was significantly greater with abrocitinib 200 mg than placebo (nominal p < 0.001) across all subgroups. Clinically meaningful differences were observed between abrocitinib and dupilumab for most evaluated endpoints across several subgroups, including in patients who failed or were intolerant to prior systemic therapy.
Conclusions
Abrocitinib provided rapid and substantially greater improvements in skin clearance and quality of life compared with placebo and dupilumab in subgroups of patients with severe and/or difficult-to-treat AD. These findings support the use of abrocitinib for severe and/or difficult-to-treat AD.
期刊介绍:
The American Journal of Clinical Dermatology is dedicated to evidence-based therapy and effective patient management in dermatology. It publishes critical review articles and clinically focused original research covering comprehensive aspects of dermatological conditions. The journal enhances visibility and educational value through features like Key Points summaries, plain language summaries, and various digital elements, ensuring accessibility and depth for a diverse readership.


 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
