{"title":"Colon Cancer Risk Following Intestinal <i>Clostridioides difficile</i> Infection: A Longitudinal Cohort Study.","authors":"David A Geier, Mark R Geier","doi":"10.14740/jocmr4919","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>The gut microbiome may play an important role in the etiology and progression of colon cancer. The present hypothesis-testing study compared the colon cancer incidence rate among adults diagnosed with intestinal <i>Clostridioides</i> (formerly <i>Clostridium) difficile</i> (Cdiff) (the Cdiff cohort) to adults not diagnosed with intestinal Cdiff infection (the non-Cdiff cohort).</p><p><strong>Methods: </strong>De-identified eligibility and claim healthcare records within the Independent Healthcare Research Database (IHRD) from a longitudinal cohort of adults (the overall cohort) enrolled in the Florida Medicaid system between 1990 through 2012 were examined. Adults with ≥ 8 outpatient office visits over 8 years of continuous eligibility were examined. There were 964 adults in the Cdiff cohort and 292,136 adults in the non-Cdiff cohort. Frequency and Cox proportional hazards models were utilized.</p><p><strong>Results: </strong>Colon cancer incidence rate in the non-Cdiff cohort remained relatively uniform over the entire study period, whereas a marked increase was observed in the Cdiff cohort within the first 4 years of a Cdiff diagnosis. Colon cancer incidence was significantly increased (about 2.7-fold) in the Cdiff cohort (3.11 per 1,000 person-years) compared to the non-Cdiff cohort (1.16 per 1,000 person-years). Adjustments for gender, age, residency, birthdate, colonoscopy screening, family history of cancer, and personal history of tobacco abuse, alcohol abuse/dependence, drug abuse/dependence, and overweight/obesity, as well as consideration of diagnostic status for ulcerative and infection colitis, immunodeficiency, and personal history of cancer did not significantly change the observed results.</p><p><strong>Conclusions: </strong>This is the first epidemiological study associating Cdiff with an increased risk for colon cancer. Future studies should further evaluate this relationship.</p>","PeriodicalId":15431,"journal":{"name":"Journal of Clinical Medicine Research","volume":"15 6","pages":"310-320"},"PeriodicalIF":0.0000,"publicationDate":"2023-06-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/74/7b/jocmr-15-310.PMC10332880.pdf","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Clinical Medicine Research","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.14740/jocmr4919","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Background: The gut microbiome may play an important role in the etiology and progression of colon cancer. The present hypothesis-testing study compared the colon cancer incidence rate among adults diagnosed with intestinal Clostridioides (formerly Clostridium) difficile (Cdiff) (the Cdiff cohort) to adults not diagnosed with intestinal Cdiff infection (the non-Cdiff cohort).
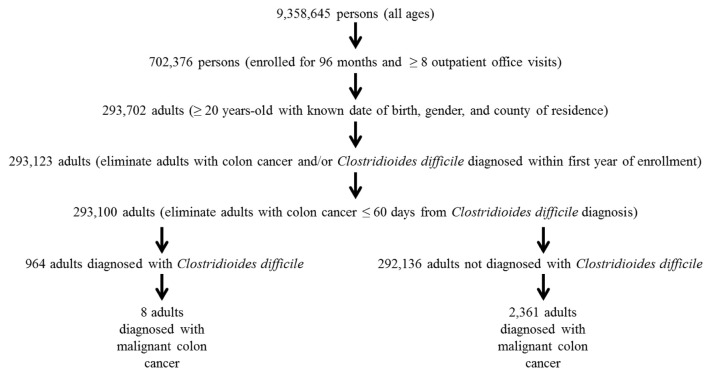
Methods: De-identified eligibility and claim healthcare records within the Independent Healthcare Research Database (IHRD) from a longitudinal cohort of adults (the overall cohort) enrolled in the Florida Medicaid system between 1990 through 2012 were examined. Adults with ≥ 8 outpatient office visits over 8 years of continuous eligibility were examined. There were 964 adults in the Cdiff cohort and 292,136 adults in the non-Cdiff cohort. Frequency and Cox proportional hazards models were utilized.
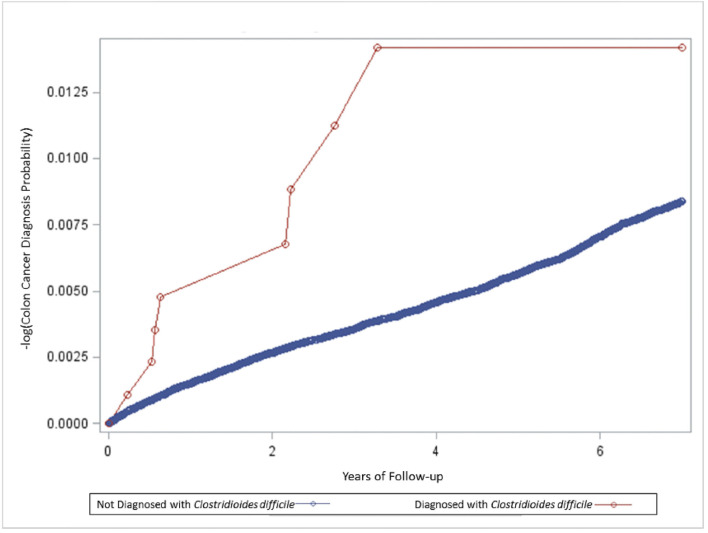
Results: Colon cancer incidence rate in the non-Cdiff cohort remained relatively uniform over the entire study period, whereas a marked increase was observed in the Cdiff cohort within the first 4 years of a Cdiff diagnosis. Colon cancer incidence was significantly increased (about 2.7-fold) in the Cdiff cohort (3.11 per 1,000 person-years) compared to the non-Cdiff cohort (1.16 per 1,000 person-years). Adjustments for gender, age, residency, birthdate, colonoscopy screening, family history of cancer, and personal history of tobacco abuse, alcohol abuse/dependence, drug abuse/dependence, and overweight/obesity, as well as consideration of diagnostic status for ulcerative and infection colitis, immunodeficiency, and personal history of cancer did not significantly change the observed results.
Conclusions: This is the first epidemiological study associating Cdiff with an increased risk for colon cancer. Future studies should further evaluate this relationship.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
