Hannah C McCausland, Charlotte J Hagerman, Marny M Ehmann, Meghan L Butryn
{"title":"Understanding the relationship between subclinical depressive symptoms and physical activity in behavioral weight loss treatment.","authors":"Hannah C McCausland, Charlotte J Hagerman, Marny M Ehmann, Meghan L Butryn","doi":"10.1002/osp4.661","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Many adults with overweight or obesity experience subclinical symptoms of depression, but little is known about how such symptoms are associated with physical activity (PA) or the experience of PA during behavioral weight loss (BWL) treatment.</p><p><strong>Methods: </strong>In the current study, adults recruited from the community (N = 320) received 18 months of group-based BWL treatment and wore accelerometers at months 0, 6, and 18 to objectively measure PA. Participants with a mood disorder that was not well controlled were not eligible for the study and were referred for individual treatment. Depressive symptoms, PA barriers, discomfort avoidance, and self-control were self-reported with validated measures.</p><p><strong>Results: </strong>At baseline, the majority of participants indicated some depressive symptoms, mostly at subclinical levels. Results of multilevel models suggest that depressive symptoms were not significantly associated with concurrent measures of PA engagement (minutes/week) or sedentary behavior (minutes/week) at a given time point (i.e., baseline, 6 months, or 18 months). Results of cross-level interactions suggest that baseline depressive symptoms did not moderate the change in PA or sedentary behavior across time. Concurrent depressive symptoms and PA barriers were significantly and positively associated at a given time point (i.e., baseline, 6 months, or 18 months); however, baseline depressive symptoms did not moderate the improvement in perceived PA barriers across time. At baseline, higher discomfort avoidance and lower self-control each independently and partially mediated the relationship between depressive symptoms and PA barriers.</p><p><strong>Conclusion: </strong>Results suggest that, among BWL samples in which most participants do not have clinically significant depressive symptoms, the likelihood of adopting and sustaining PA does not depend on the extent of depressive symptoms, but those with elevated symptoms may benefit from approaches that address their perception that engaging in PA is especially challenging.</p>","PeriodicalId":19448,"journal":{"name":"Obesity Science & Practice","volume":"9 4","pages":"364-375"},"PeriodicalIF":1.9000,"publicationDate":"2023-01-17","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/cc/8f/OSP4-9-364.PMC10399524.pdf","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Obesity Science & Practice","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1002/osp4.661","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2023/8/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"ENDOCRINOLOGY & METABOLISM","Score":null,"Total":0}
引用次数: 0
Abstract
Introduction: Many adults with overweight or obesity experience subclinical symptoms of depression, but little is known about how such symptoms are associated with physical activity (PA) or the experience of PA during behavioral weight loss (BWL) treatment.
Methods: In the current study, adults recruited from the community (N = 320) received 18 months of group-based BWL treatment and wore accelerometers at months 0, 6, and 18 to objectively measure PA. Participants with a mood disorder that was not well controlled were not eligible for the study and were referred for individual treatment. Depressive symptoms, PA barriers, discomfort avoidance, and self-control were self-reported with validated measures.
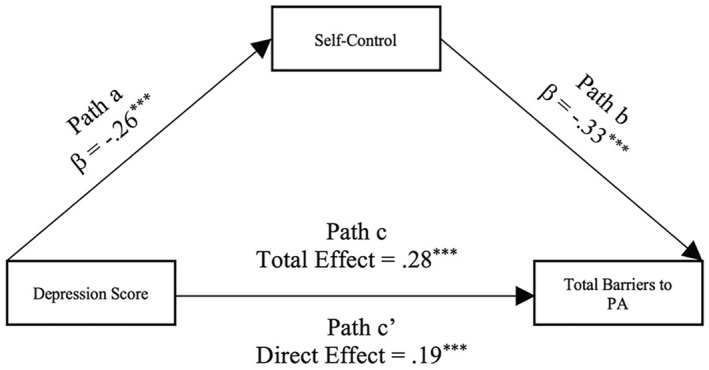
Results: At baseline, the majority of participants indicated some depressive symptoms, mostly at subclinical levels. Results of multilevel models suggest that depressive symptoms were not significantly associated with concurrent measures of PA engagement (minutes/week) or sedentary behavior (minutes/week) at a given time point (i.e., baseline, 6 months, or 18 months). Results of cross-level interactions suggest that baseline depressive symptoms did not moderate the change in PA or sedentary behavior across time. Concurrent depressive symptoms and PA barriers were significantly and positively associated at a given time point (i.e., baseline, 6 months, or 18 months); however, baseline depressive symptoms did not moderate the improvement in perceived PA barriers across time. At baseline, higher discomfort avoidance and lower self-control each independently and partially mediated the relationship between depressive symptoms and PA barriers.
Conclusion: Results suggest that, among BWL samples in which most participants do not have clinically significant depressive symptoms, the likelihood of adopting and sustaining PA does not depend on the extent of depressive symptoms, but those with elevated symptoms may benefit from approaches that address their perception that engaging in PA is especially challenging.





 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
