Alessandra Chinè, Marco Reschini, Gianfranco Fornelli, Ludovica Basili, Andrea Busnelli, Paola Viganò, Ludovico Muzii, Edgardo Somigliana
{"title":"Low ovarian reserve and risk of miscarriage in pregnancies derived from assisted reproductive technology.","authors":"Alessandra Chinè, Marco Reschini, Gianfranco Fornelli, Ludovica Basili, Andrea Busnelli, Paola Viganò, Ludovico Muzii, Edgardo Somigliana","doi":"10.1093/hropen/hoad026","DOIUrl":null,"url":null,"abstract":"<p><strong>Study question: </strong>Do low levels of anti-Müllerian hormone (AMH) or antral follicle count (AFC) properly predict miscarriage in young women conceiving with ART?</p><p><strong>Summary answer: </strong>Low ovarian reserve, as indicated by AMH or AFC, is not associated with miscarriage in young women conceiving with ART.</p><p><strong>What is known already: </strong>Presently, the impact of low ovarian reserve on the risk of miscarriage remains controversial. Some studies have reported an association between serum AMH levels and AFC and miscarriage, but others have failed to confirm these findings. The main limitation that undermines the reliability and consistency of the results is the confounding effect of female age. Indeed, after 35 years of age, on the one hand, the risk of miscarriage starts increasing because of impaired oocyte quality while, on the other, the physiological decline in AMH and AFC levels continues, thus hampering the possibility to properly explore the real effects of reduced ovarian reserve. Indeed, the two processes, i.e. the gradual loss of resting primordial follicles and the loss of oocyte quality, progress in parallel. In other words, the older the woman becomes, the higher is the risk of miscarriage, but one cannot distinguish between the effects of biological aging on oocyte quality and those mediated by a lower ovarian reserve.</p><p><strong>Study design size duration: </strong>The present retrospective monocentric cohort study was carried out at Fondazione IRCSS Ca Granda Ospedale Maggiore Policlinico, Milan. All women referred to the ART Unit between 2014 and 2021 and who underwent either conventional IVF (c-IVF), ICSI, or IUI were reviewed. Only women younger than 35 were eligible because, up to this age, the risk of miscarriage is steady and not strictly related to age.</p><p><strong>Participants/materials setting methods: </strong>Women younger than 35 who achieved a singleton clinical pregnancy with c-IVF, ICSI, or IUI were selected. Women with patent causes of recurrent miscarriage were excluded, as well as those undergoing pregnancy termination for fetal or medical causes. Women who did and did not have a pregnancy loss before 20 weeks' gestation were compared. Detailed information was obtained from charts of the consulting patients. ART procedures were performed according to the standardized policy of our Unit. All women underwent serum AMH measurement and a transvaginal assessment of AFC prior to initiation of treatment. AMH levels were measured by a commercially available ELISA assay. To assess AFC, all identifiable antral follicles 2-10 mm in diameter at ultrasound were recorded. The primary outcome was the risk of miscarriage for women with serum AMH levels below 5 pmol/l.</p><p><strong>Main results and the role of chance: </strong>There were 538 women were included, of whom 92 (17%) had a miscarriage. The areas under the ROC curves for prediction of miscarriage based on AMH levels and AFC were 0.51 (95% CI: 0.45-0.58) and 0.52 (95% CI: 0.45-0.59), respectively. The odds ratio (OR) of miscarriage for women with serum AMH levels below 5.0 pmol/l was 1.10 (95% CI: 0.51-2.36); the adjusted OR was 1.12 (95% CI: 0.51-2.45). Analyses were repeated considering other thresholds for AMH (2.9, 3.6 and 7.9 pmol/l) and for AFC (thresholds of 7 and 10). No associations emerged.</p><p><strong>Limitations reasons for caution: </strong>The retrospective design of the study hampered the collection of more precise but potentially relevant clinical information of the couples. We did not exclude women suffering from PCOS, a condition possibly associated with miscarriage. Moreover, the baseline characteristics of women who did and did not have a miscarriage differed in some characteristics. Thus, we adjusted the OR using a multivariate analysis, but we cannot fully exclude residual confounding effects. Finally, our results cannot be inferred to women older than 35. The mechanisms causing premature exhaustion of ovarian reserve may be different in younger and older women and this may lead to a different impact on the risk of miscarriage.</p><p><strong>Wider implications of the findings: </strong>Women embarking on ART with low ovarian reserve should be informed of their likely poor response to ovarian stimulation but can be reassured that, if conception occurs, their risk of miscarriage is not increased.</p><p><strong>Study funding/competing interests: </strong>This study was partially funded by Italian Ministry of Health-Current research IRCCS. E.S. reports grants from Ferring and honoraria for lectures from Merck-Serono and Gedeon-Richter. All the other authors do not have any competing interest to declare.</p><p><strong>Trial registration number: </strong>N/A.</p>","PeriodicalId":73264,"journal":{"name":"Human reproduction open","volume":"2023 3","pages":"hoad026"},"PeriodicalIF":11.1000,"publicationDate":"2023-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/83/c4/hoad026.PMC10243845.pdf","citationCount":"1","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Human reproduction open","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1093/hropen/hoad026","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"OBSTETRICS & GYNECOLOGY","Score":null,"Total":0}
引用次数: 1
Abstract
Study question: Do low levels of anti-Müllerian hormone (AMH) or antral follicle count (AFC) properly predict miscarriage in young women conceiving with ART?
Summary answer: Low ovarian reserve, as indicated by AMH or AFC, is not associated with miscarriage in young women conceiving with ART.
What is known already: Presently, the impact of low ovarian reserve on the risk of miscarriage remains controversial. Some studies have reported an association between serum AMH levels and AFC and miscarriage, but others have failed to confirm these findings. The main limitation that undermines the reliability and consistency of the results is the confounding effect of female age. Indeed, after 35 years of age, on the one hand, the risk of miscarriage starts increasing because of impaired oocyte quality while, on the other, the physiological decline in AMH and AFC levels continues, thus hampering the possibility to properly explore the real effects of reduced ovarian reserve. Indeed, the two processes, i.e. the gradual loss of resting primordial follicles and the loss of oocyte quality, progress in parallel. In other words, the older the woman becomes, the higher is the risk of miscarriage, but one cannot distinguish between the effects of biological aging on oocyte quality and those mediated by a lower ovarian reserve.
Study design size duration: The present retrospective monocentric cohort study was carried out at Fondazione IRCSS Ca Granda Ospedale Maggiore Policlinico, Milan. All women referred to the ART Unit between 2014 and 2021 and who underwent either conventional IVF (c-IVF), ICSI, or IUI were reviewed. Only women younger than 35 were eligible because, up to this age, the risk of miscarriage is steady and not strictly related to age.
Participants/materials setting methods: Women younger than 35 who achieved a singleton clinical pregnancy with c-IVF, ICSI, or IUI were selected. Women with patent causes of recurrent miscarriage were excluded, as well as those undergoing pregnancy termination for fetal or medical causes. Women who did and did not have a pregnancy loss before 20 weeks' gestation were compared. Detailed information was obtained from charts of the consulting patients. ART procedures were performed according to the standardized policy of our Unit. All women underwent serum AMH measurement and a transvaginal assessment of AFC prior to initiation of treatment. AMH levels were measured by a commercially available ELISA assay. To assess AFC, all identifiable antral follicles 2-10 mm in diameter at ultrasound were recorded. The primary outcome was the risk of miscarriage for women with serum AMH levels below 5 pmol/l.
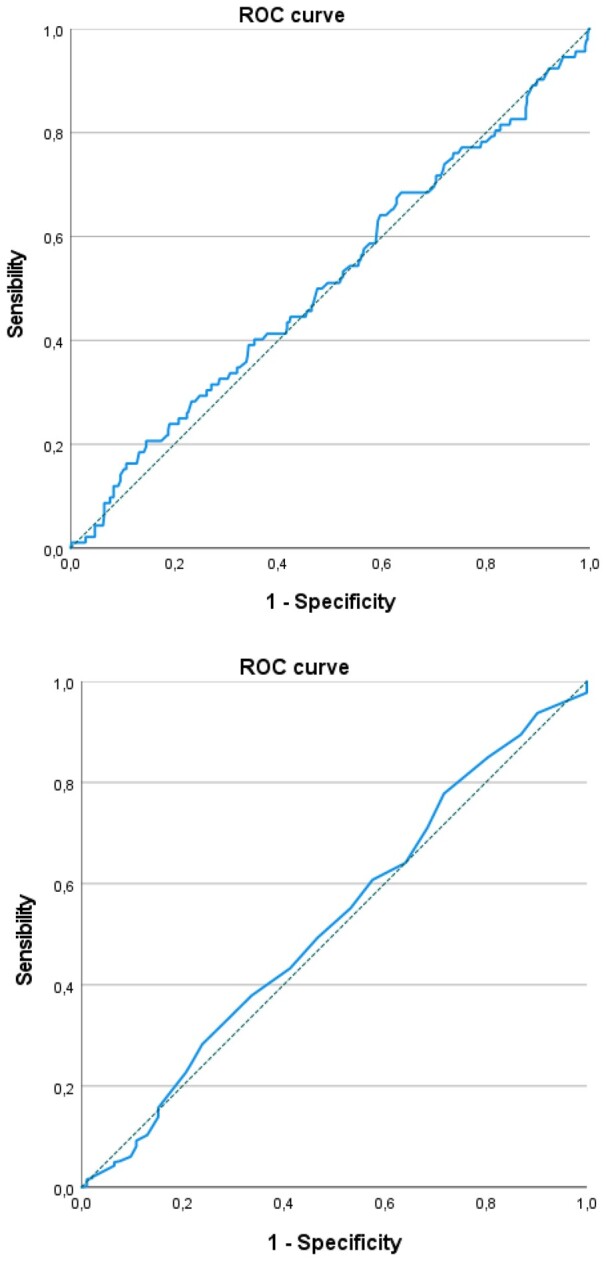
Main results and the role of chance: There were 538 women were included, of whom 92 (17%) had a miscarriage. The areas under the ROC curves for prediction of miscarriage based on AMH levels and AFC were 0.51 (95% CI: 0.45-0.58) and 0.52 (95% CI: 0.45-0.59), respectively. The odds ratio (OR) of miscarriage for women with serum AMH levels below 5.0 pmol/l was 1.10 (95% CI: 0.51-2.36); the adjusted OR was 1.12 (95% CI: 0.51-2.45). Analyses were repeated considering other thresholds for AMH (2.9, 3.6 and 7.9 pmol/l) and for AFC (thresholds of 7 and 10). No associations emerged.
Limitations reasons for caution: The retrospective design of the study hampered the collection of more precise but potentially relevant clinical information of the couples. We did not exclude women suffering from PCOS, a condition possibly associated with miscarriage. Moreover, the baseline characteristics of women who did and did not have a miscarriage differed in some characteristics. Thus, we adjusted the OR using a multivariate analysis, but we cannot fully exclude residual confounding effects. Finally, our results cannot be inferred to women older than 35. The mechanisms causing premature exhaustion of ovarian reserve may be different in younger and older women and this may lead to a different impact on the risk of miscarriage.
Wider implications of the findings: Women embarking on ART with low ovarian reserve should be informed of their likely poor response to ovarian stimulation but can be reassured that, if conception occurs, their risk of miscarriage is not increased.
Study funding/competing interests: This study was partially funded by Italian Ministry of Health-Current research IRCCS. E.S. reports grants from Ferring and honoraria for lectures from Merck-Serono and Gedeon-Richter. All the other authors do not have any competing interest to declare.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
