{"title":"A Case of Non-Tachycardic Atrial Fibrillation Whose Left Ventricular Systolic Dysfunction Improved After Catheter Ablation.","authors":"Asami Yamashita, Shunsuke Kiuchi, Takanori Ikeda","doi":"10.14740/jocmr4908","DOIUrl":null,"url":null,"abstract":"<p><p>It is difficult to identify the causes and optimal treatment of heart failure (HF) in patients with atrial fibrillation (AF) and HF with reduced ejection fraction (EF) (HFrEF). Tachyarrhythmia can cause left ventricular (LV) systolic dysfunction called tachycardia-induced cardiomyopathy (TIC). In patients with TIC, conversion to sinus rhythm may lead to improvement in LV systolic dysfunction. However, it is unclear whether we should try to convert patients with AF without tachycardia to sinus rhythm. A 46-year-old man with chronic AF and HFrEF came to our hospital. His New York Heart Association (NYHA) classification was class II. The blood test showed a brain natriuretic peptide of 105 pg/mL. Electrocardiogram (ECG) and 24-h ECG showed AF without tachycardia. Transthoracic echocardiography (TTE) showed left atrial (LA) dilatation, LV dilatation, and diffuse LV hypokinesis (EF was 40%). Although he was optimized medically, NYHA classification II persisted. Therefore, he underwent direct current cardioversion and catheter ablation. After his AF converted to a sinus rhythm of heart rate (HR) 60 - 70 beats per minute (bpm), TTE showed improvement in LV systolic dysfunction. We gradually reduced oral medications for arrhythmia and HF. We subsequently succeeded in discontinuing all medications 1 year after catheter ablation. TTE performed between 1 and 2 years after catheter ablation showed normal LV function and normal cardiac size. During the 3 years of follow-up, there was no recurrence of AF, and he was not readmitted to the hospital. This patient showed the effectiveness of converting AF to sinus rhythm in patients without tachycardia.</p>","PeriodicalId":15431,"journal":{"name":"Journal of Clinical Medicine Research","volume":"15 5","pages":"274-278"},"PeriodicalIF":0.0000,"publicationDate":"2023-05-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/de/4d/jocmr-15-274.PMC10251699.pdf","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Clinical Medicine Research","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.14740/jocmr4908","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
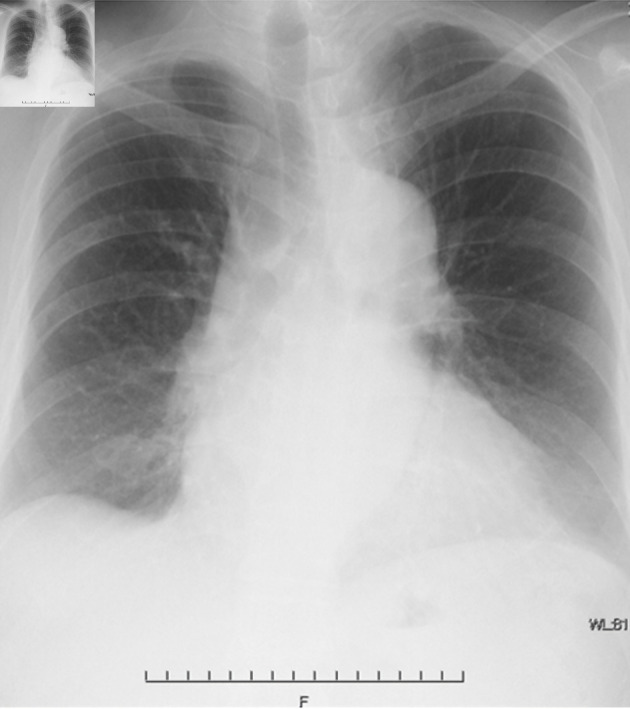
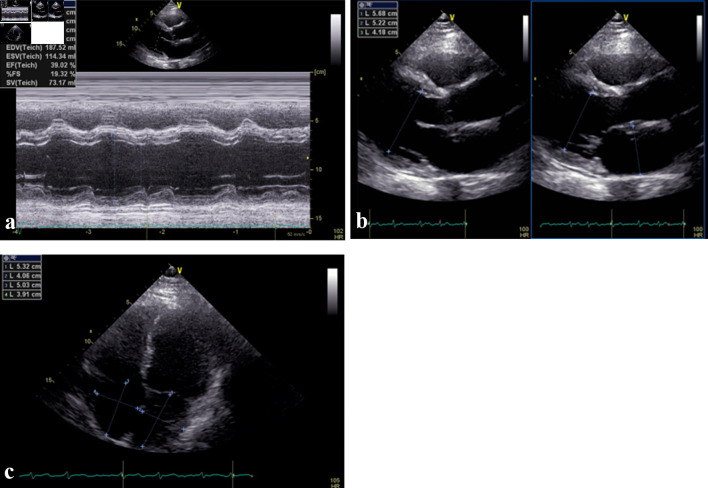
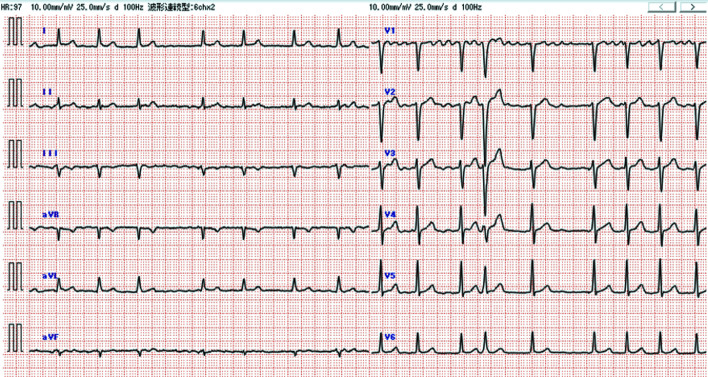
It is difficult to identify the causes and optimal treatment of heart failure (HF) in patients with atrial fibrillation (AF) and HF with reduced ejection fraction (EF) (HFrEF). Tachyarrhythmia can cause left ventricular (LV) systolic dysfunction called tachycardia-induced cardiomyopathy (TIC). In patients with TIC, conversion to sinus rhythm may lead to improvement in LV systolic dysfunction. However, it is unclear whether we should try to convert patients with AF without tachycardia to sinus rhythm. A 46-year-old man with chronic AF and HFrEF came to our hospital. His New York Heart Association (NYHA) classification was class II. The blood test showed a brain natriuretic peptide of 105 pg/mL. Electrocardiogram (ECG) and 24-h ECG showed AF without tachycardia. Transthoracic echocardiography (TTE) showed left atrial (LA) dilatation, LV dilatation, and diffuse LV hypokinesis (EF was 40%). Although he was optimized medically, NYHA classification II persisted. Therefore, he underwent direct current cardioversion and catheter ablation. After his AF converted to a sinus rhythm of heart rate (HR) 60 - 70 beats per minute (bpm), TTE showed improvement in LV systolic dysfunction. We gradually reduced oral medications for arrhythmia and HF. We subsequently succeeded in discontinuing all medications 1 year after catheter ablation. TTE performed between 1 and 2 years after catheter ablation showed normal LV function and normal cardiac size. During the 3 years of follow-up, there was no recurrence of AF, and he was not readmitted to the hospital. This patient showed the effectiveness of converting AF to sinus rhythm in patients without tachycardia.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
