Jeroen Hoogland, Toshihiko Takada, Maarten van Smeden, Maroeska M Rovers, An I de Sutter, Daniel Merenstein, Laurent Kaiser, Helena Liira, Paul Little, Heiner C Bucher, Karel G M Moons, Johannes B Reitsma, Roderick P Venekamp
{"title":"临床诊断为急性鼻窦炎的成人的预后和抗生素获益预测:个体参与者数据荟萃分析","authors":"Jeroen Hoogland, Toshihiko Takada, Maarten van Smeden, Maroeska M Rovers, An I de Sutter, Daniel Merenstein, Laurent Kaiser, Helena Liira, Paul Little, Heiner C Bucher, Karel G M Moons, Johannes B Reitsma, Roderick P Venekamp","doi":"10.1186/s41512-023-00154-0","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>A previous individual participant data meta-analysis (IPD-MA) of antibiotics for adults with clinically diagnosed acute rhinosinusitis (ARS) showed a marginal overall effect of antibiotics, but was unable to identify patients that are most likely to benefit from antibiotics when applying conventional (i.e. univariable or one-variable-at-a-time) subgroup analysis. We updated the systematic review and investigated whether multivariable prediction of patient-level prognosis and antibiotic treatment effect may lead to more tailored treatment assignment in adults presenting to primary care with ARS.</p><p><strong>Methods: </strong>An IPD-MA of nine double-blind placebo-controlled trials of antibiotic treatment (n=2539) was conducted, with the probability of being cured at 8-15 days as the primary outcome. A logistic mixed effects model was developed to predict the probability of being cured based on demographic characteristics, signs and symptoms, and antibiotic treatment assignment. Predictive performance was quantified based on internal-external cross-validation in terms of calibration and discrimination performance, overall model fit, and the accuracy of individual predictions.</p><p><strong>Results: </strong>Results indicate that the prognosis with respect to risk of cure could not be reliably predicted (c-statistic 0.58 and Brier score 0.24). Similarly, patient-level treatment effect predictions did not reliably distinguish between those that did and did not benefit from antibiotics (c-for-benefit 0.50).</p><p><strong>Conclusions: </strong>In conclusion, multivariable prediction based on patient demographics and common signs and symptoms did not reliably predict the patient-level probability of cure and antibiotic effect in this IPD-MA. Therefore, these characteristics cannot be expected to reliably distinguish those that do and do not benefit from antibiotics in adults presenting to primary care with ARS.</p>","PeriodicalId":72800,"journal":{"name":"Diagnostic and prognostic research","volume":"7 1","pages":"16"},"PeriodicalIF":2.6000,"publicationDate":"2023-09-05","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10478354/pdf/","citationCount":"0","resultStr":"{\"title\":\"Prognosis and prediction of antibiotic benefit in adults with clinically diagnosed acute rhinosinusitis: an individual participant data meta-analysis.\",\"authors\":\"Jeroen Hoogland, Toshihiko Takada, Maarten van Smeden, Maroeska M Rovers, An I de Sutter, Daniel Merenstein, Laurent Kaiser, Helena Liira, Paul Little, Heiner C Bucher, Karel G M Moons, Johannes B Reitsma, Roderick P Venekamp\",\"doi\":\"10.1186/s41512-023-00154-0\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>A previous individual participant data meta-analysis (IPD-MA) of antibiotics for adults with clinically diagnosed acute rhinosinusitis (ARS) showed a marginal overall effect of antibiotics, but was unable to identify patients that are most likely to benefit from antibiotics when applying conventional (i.e. univariable or one-variable-at-a-time) subgroup analysis. We updated the systematic review and investigated whether multivariable prediction of patient-level prognosis and antibiotic treatment effect may lead to more tailored treatment assignment in adults presenting to primary care with ARS.</p><p><strong>Methods: </strong>An IPD-MA of nine double-blind placebo-controlled trials of antibiotic treatment (n=2539) was conducted, with the probability of being cured at 8-15 days as the primary outcome. A logistic mixed effects model was developed to predict the probability of being cured based on demographic characteristics, signs and symptoms, and antibiotic treatment assignment. Predictive performance was quantified based on internal-external cross-validation in terms of calibration and discrimination performance, overall model fit, and the accuracy of individual predictions.</p><p><strong>Results: </strong>Results indicate that the prognosis with respect to risk of cure could not be reliably predicted (c-statistic 0.58 and Brier score 0.24). Similarly, patient-level treatment effect predictions did not reliably distinguish between those that did and did not benefit from antibiotics (c-for-benefit 0.50).</p><p><strong>Conclusions: </strong>In conclusion, multivariable prediction based on patient demographics and common signs and symptoms did not reliably predict the patient-level probability of cure and antibiotic effect in this IPD-MA. Therefore, these characteristics cannot be expected to reliably distinguish those that do and do not benefit from antibiotics in adults presenting to primary care with ARS.</p>\",\"PeriodicalId\":72800,\"journal\":{\"name\":\"Diagnostic and prognostic research\",\"volume\":\"7 1\",\"pages\":\"16\"},\"PeriodicalIF\":2.6000,\"publicationDate\":\"2023-09-05\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10478354/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Diagnostic and prognostic research\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1186/s41512-023-00154-0\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Diagnostic and prognostic research","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1186/s41512-023-00154-0","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
Prognosis and prediction of antibiotic benefit in adults with clinically diagnosed acute rhinosinusitis: an individual participant data meta-analysis.
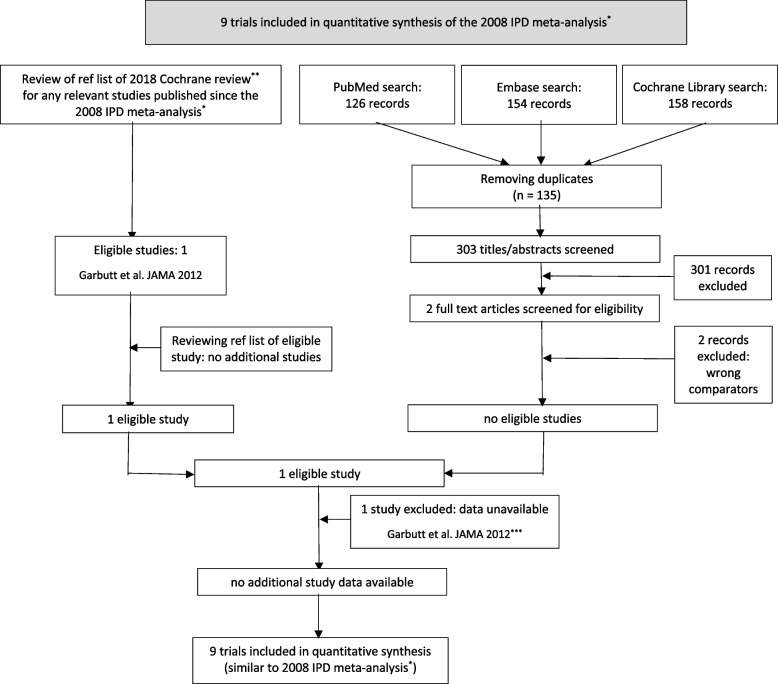
Background: A previous individual participant data meta-analysis (IPD-MA) of antibiotics for adults with clinically diagnosed acute rhinosinusitis (ARS) showed a marginal overall effect of antibiotics, but was unable to identify patients that are most likely to benefit from antibiotics when applying conventional (i.e. univariable or one-variable-at-a-time) subgroup analysis. We updated the systematic review and investigated whether multivariable prediction of patient-level prognosis and antibiotic treatment effect may lead to more tailored treatment assignment in adults presenting to primary care with ARS.
Methods: An IPD-MA of nine double-blind placebo-controlled trials of antibiotic treatment (n=2539) was conducted, with the probability of being cured at 8-15 days as the primary outcome. A logistic mixed effects model was developed to predict the probability of being cured based on demographic characteristics, signs and symptoms, and antibiotic treatment assignment. Predictive performance was quantified based on internal-external cross-validation in terms of calibration and discrimination performance, overall model fit, and the accuracy of individual predictions.
Results: Results indicate that the prognosis with respect to risk of cure could not be reliably predicted (c-statistic 0.58 and Brier score 0.24). Similarly, patient-level treatment effect predictions did not reliably distinguish between those that did and did not benefit from antibiotics (c-for-benefit 0.50).
Conclusions: In conclusion, multivariable prediction based on patient demographics and common signs and symptoms did not reliably predict the patient-level probability of cure and antibiotic effect in this IPD-MA. Therefore, these characteristics cannot be expected to reliably distinguish those that do and do not benefit from antibiotics in adults presenting to primary care with ARS.



 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
