Kristen Glenister, Tessa Archbold, Anna Moran, David Kidd, Sue Wilson, Rebecca Disler
{"title":"从患者和卫生专业人员的角度理解澳大利亚农村地区可能避免的住院:定性研究和逻辑模型。","authors":"Kristen Glenister, Tessa Archbold, Anna Moran, David Kidd, Sue Wilson, Rebecca Disler","doi":"10.1136/ihj-2021-000124","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Potentially avoidable hospitalisations (PAHs) are proxy measures of effective primary care at a population level. PAHs are higher in rural and disadvantaged areas. This qualitative study sought a deeper understanding of PAHs for chronic health conditions in a rural context from the perspectives of patients and health professionals, and aimed to develop a logic model for rural health services to identify intervention targets.</p><p><strong>Methods: </strong>Patients with chronic obstructive pulmonary disease, congestive cardiac failure or type 2 diabetes, admitted to a rural hospital in Australia and local health professionals were invited to participate in interviews in late 2019. Semistructured interviews were recorded, transcribed verbatim and thematically analysed. Themes were mapped against a programme logic model developed in a similar study.</p><p><strong>Results: </strong>patients and 16 health professionals participated. The logic model encompassed patient level (knowledge, skills, health status), provider level (workforce availability, attributes) and system level (clinical pathways) contexts. These contexts influenced key mechanisms of relationships, continuity of care and capacity to offer services. Outcomes included responsive and timely access to care, improved clinical outcomes and resource use. Themes that did not readily map to the logic model included socioeconomic disadvantage and healthcare costs, which influenced affordability and equity of access.</p><p><strong>Conclusion: </strong>Patients' complex health and social circumstance, health service access and unclear care pathways were strong themes associated with PAH in this rural context. Patient, provider and system contexts influencing key mechanisms and outcomes need to be understood when designing solutions to address PAHs in rural settings. Ideally, interventions should address the cost of healthcare alongside interventions to enhance relationships, continuity of care and capacity to offer services.</p>","PeriodicalId":73393,"journal":{"name":"Integrated healthcare journal","volume":"4 1","pages":"e000124"},"PeriodicalIF":0.0000,"publicationDate":"2022-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/89/71/ihj-2021-000124.PMC10241033.pdf","citationCount":"0","resultStr":"{\"title\":\"Understanding potentially avoidable hospitalisations in a rural Australian setting from the perspectives of patients and health professionals: a qualitative study and logic model.\",\"authors\":\"Kristen Glenister, Tessa Archbold, Anna Moran, David Kidd, Sue Wilson, Rebecca Disler\",\"doi\":\"10.1136/ihj-2021-000124\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Potentially avoidable hospitalisations (PAHs) are proxy measures of effective primary care at a population level. PAHs are higher in rural and disadvantaged areas. This qualitative study sought a deeper understanding of PAHs for chronic health conditions in a rural context from the perspectives of patients and health professionals, and aimed to develop a logic model for rural health services to identify intervention targets.</p><p><strong>Methods: </strong>Patients with chronic obstructive pulmonary disease, congestive cardiac failure or type 2 diabetes, admitted to a rural hospital in Australia and local health professionals were invited to participate in interviews in late 2019. Semistructured interviews were recorded, transcribed verbatim and thematically analysed. Themes were mapped against a programme logic model developed in a similar study.</p><p><strong>Results: </strong>patients and 16 health professionals participated. The logic model encompassed patient level (knowledge, skills, health status), provider level (workforce availability, attributes) and system level (clinical pathways) contexts. These contexts influenced key mechanisms of relationships, continuity of care and capacity to offer services. Outcomes included responsive and timely access to care, improved clinical outcomes and resource use. Themes that did not readily map to the logic model included socioeconomic disadvantage and healthcare costs, which influenced affordability and equity of access.</p><p><strong>Conclusion: </strong>Patients' complex health and social circumstance, health service access and unclear care pathways were strong themes associated with PAH in this rural context. Patient, provider and system contexts influencing key mechanisms and outcomes need to be understood when designing solutions to address PAHs in rural settings. Ideally, interventions should address the cost of healthcare alongside interventions to enhance relationships, continuity of care and capacity to offer services.</p>\",\"PeriodicalId\":73393,\"journal\":{\"name\":\"Integrated healthcare journal\",\"volume\":\"4 1\",\"pages\":\"e000124\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2022-01-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/89/71/ihj-2021-000124.PMC10241033.pdf\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Integrated healthcare journal\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1136/ihj-2021-000124\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Integrated healthcare journal","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1136/ihj-2021-000124","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
Understanding potentially avoidable hospitalisations in a rural Australian setting from the perspectives of patients and health professionals: a qualitative study and logic model.
Background: Potentially avoidable hospitalisations (PAHs) are proxy measures of effective primary care at a population level. PAHs are higher in rural and disadvantaged areas. This qualitative study sought a deeper understanding of PAHs for chronic health conditions in a rural context from the perspectives of patients and health professionals, and aimed to develop a logic model for rural health services to identify intervention targets.
Methods: Patients with chronic obstructive pulmonary disease, congestive cardiac failure or type 2 diabetes, admitted to a rural hospital in Australia and local health professionals were invited to participate in interviews in late 2019. Semistructured interviews were recorded, transcribed verbatim and thematically analysed. Themes were mapped against a programme logic model developed in a similar study.
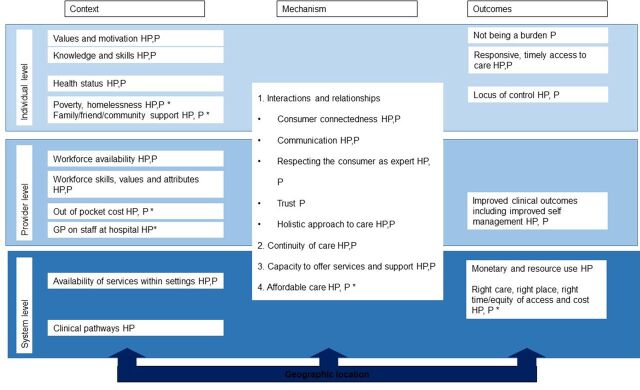
Results: patients and 16 health professionals participated. The logic model encompassed patient level (knowledge, skills, health status), provider level (workforce availability, attributes) and system level (clinical pathways) contexts. These contexts influenced key mechanisms of relationships, continuity of care and capacity to offer services. Outcomes included responsive and timely access to care, improved clinical outcomes and resource use. Themes that did not readily map to the logic model included socioeconomic disadvantage and healthcare costs, which influenced affordability and equity of access.
Conclusion: Patients' complex health and social circumstance, health service access and unclear care pathways were strong themes associated with PAH in this rural context. Patient, provider and system contexts influencing key mechanisms and outcomes need to be understood when designing solutions to address PAHs in rural settings. Ideally, interventions should address the cost of healthcare alongside interventions to enhance relationships, continuity of care and capacity to offer services.



 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
