Lars Borgen , Kjartan Aasekjær , Øyvind Werpen Skoe
{"title":"利用血管内主动脉修复作为一种微创方法——在非大学医院的九年经验","authors":"Lars Borgen , Kjartan Aasekjær , Øyvind Werpen Skoe","doi":"10.1016/j.ejro.2023.100522","DOIUrl":null,"url":null,"abstract":"<div><h3>Background</h3><p>At the introduction of endovascular aortic repair (EVAR) in 2013 in our non-university hospital, we established a quality registry to monitor our EVAR activity.</p></div><div><h3>Purpose</h3><p>To observe if we over time were able to exploit EVAR as a minimally invasive method in an elective as well as emergency setting, and to monitor our treatment quality in terms of complications, secondary interventions and mortality.</p></div><div><h3>Material and methods</h3><p>From November 2013 to March 2022, we treated 207 patients with EVAR, including six patients with rupture. Follow-up regimen was partly based on contrast-enhanced computer tomography, and partly on contrast-enhanced ultrasound in combination with plain radiography.</p></div><div><h3>Results</h3><p>During the observation period, the method of anesthesia changed from general, via spinal, to local anesthesia. The groin access changed from surgical cut down to percutaneous and the median length of postoperative stay decreased from 3 days to 1 day. EVAR on ruptured aneurysm was done for the first time in 2019. Endoleak was detected in 85 patients (42%) and 37 patients (18%) had one or more secondary interventions, of which 85% were endovascular. Estimated five-year survival was 72% in patients below 80 years of age and 45% in patients 80 years or older.</p></div><div><h3>Conclusion</h3><p>Nine years of experience enabled us to exploit EVAR’s advantages as a minimally invasive method in an elective as well as emergency setting. Complications, secondary interventions and survival rates in our low volume non-university hospital matches results from larger vascular centers.</p></div>","PeriodicalId":38076,"journal":{"name":"European Journal of Radiology Open","volume":"11 ","pages":"Article 100522"},"PeriodicalIF":2.9000,"publicationDate":"2023-12-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10493885/pdf/","citationCount":"0","resultStr":"{\"title\":\"Exploiting endovascular aortic repair as a minimally invasive method – Nine years of experience in a non-university hospital\",\"authors\":\"Lars Borgen , Kjartan Aasekjær , Øyvind Werpen Skoe\",\"doi\":\"10.1016/j.ejro.2023.100522\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<div><h3>Background</h3><p>At the introduction of endovascular aortic repair (EVAR) in 2013 in our non-university hospital, we established a quality registry to monitor our EVAR activity.</p></div><div><h3>Purpose</h3><p>To observe if we over time were able to exploit EVAR as a minimally invasive method in an elective as well as emergency setting, and to monitor our treatment quality in terms of complications, secondary interventions and mortality.</p></div><div><h3>Material and methods</h3><p>From November 2013 to March 2022, we treated 207 patients with EVAR, including six patients with rupture. Follow-up regimen was partly based on contrast-enhanced computer tomography, and partly on contrast-enhanced ultrasound in combination with plain radiography.</p></div><div><h3>Results</h3><p>During the observation period, the method of anesthesia changed from general, via spinal, to local anesthesia. The groin access changed from surgical cut down to percutaneous and the median length of postoperative stay decreased from 3 days to 1 day. EVAR on ruptured aneurysm was done for the first time in 2019. Endoleak was detected in 85 patients (42%) and 37 patients (18%) had one or more secondary interventions, of which 85% were endovascular. Estimated five-year survival was 72% in patients below 80 years of age and 45% in patients 80 years or older.</p></div><div><h3>Conclusion</h3><p>Nine years of experience enabled us to exploit EVAR’s advantages as a minimally invasive method in an elective as well as emergency setting. Complications, secondary interventions and survival rates in our low volume non-university hospital matches results from larger vascular centers.</p></div>\",\"PeriodicalId\":38076,\"journal\":{\"name\":\"European Journal of Radiology Open\",\"volume\":\"11 \",\"pages\":\"Article 100522\"},\"PeriodicalIF\":2.9000,\"publicationDate\":\"2023-12-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10493885/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"European Journal of Radiology Open\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://www.sciencedirect.com/science/article/pii/S2352047723000485\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2023/9/4 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q3\",\"JCRName\":\"RADIOLOGY, NUCLEAR MEDICINE & MEDICAL IMAGING\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"European Journal of Radiology Open","FirstCategoryId":"1085","ListUrlMain":"https://www.sciencedirect.com/science/article/pii/S2352047723000485","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2023/9/4 0:00:00","PubModel":"Epub","JCR":"Q3","JCRName":"RADIOLOGY, NUCLEAR MEDICINE & MEDICAL IMAGING","Score":null,"Total":0}
Exploiting endovascular aortic repair as a minimally invasive method – Nine years of experience in a non-university hospital
Background
At the introduction of endovascular aortic repair (EVAR) in 2013 in our non-university hospital, we established a quality registry to monitor our EVAR activity.
Purpose
To observe if we over time were able to exploit EVAR as a minimally invasive method in an elective as well as emergency setting, and to monitor our treatment quality in terms of complications, secondary interventions and mortality.
Material and methods
From November 2013 to March 2022, we treated 207 patients with EVAR, including six patients with rupture. Follow-up regimen was partly based on contrast-enhanced computer tomography, and partly on contrast-enhanced ultrasound in combination with plain radiography.
Results
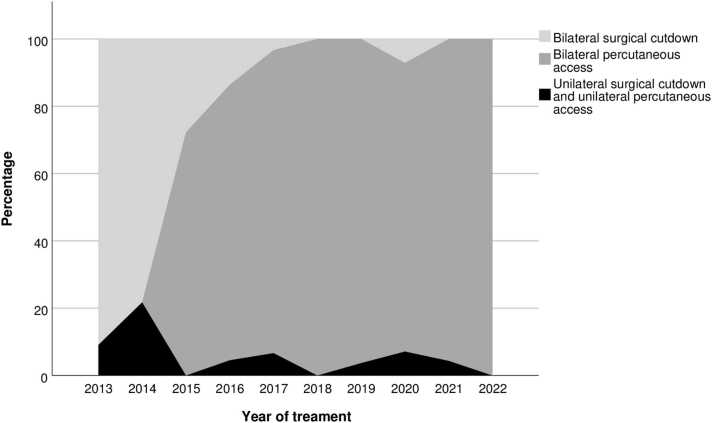
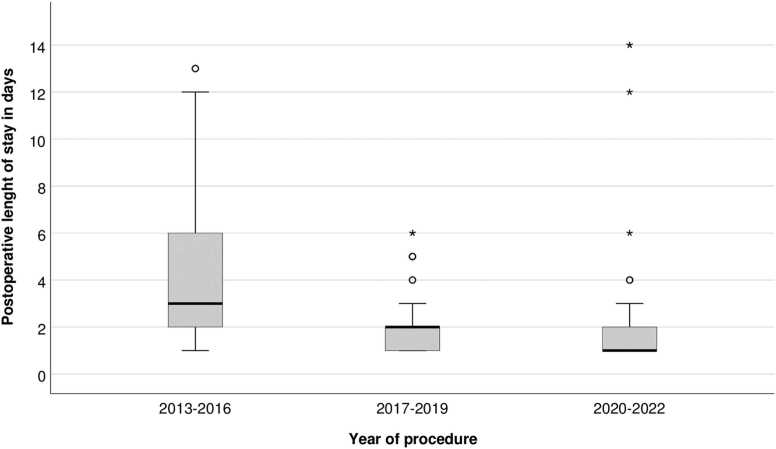
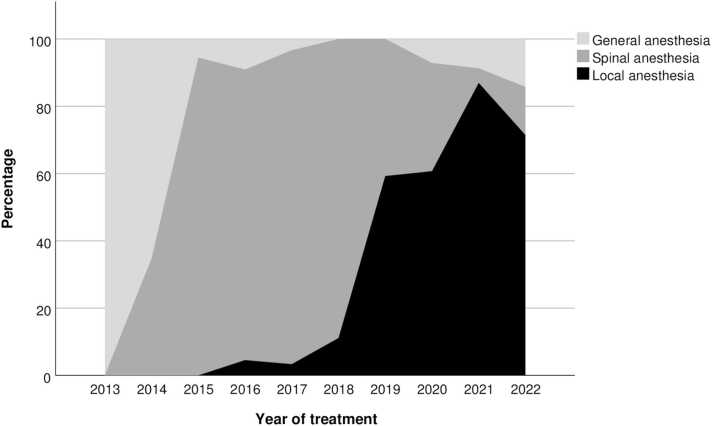
During the observation period, the method of anesthesia changed from general, via spinal, to local anesthesia. The groin access changed from surgical cut down to percutaneous and the median length of postoperative stay decreased from 3 days to 1 day. EVAR on ruptured aneurysm was done for the first time in 2019. Endoleak was detected in 85 patients (42%) and 37 patients (18%) had one or more secondary interventions, of which 85% were endovascular. Estimated five-year survival was 72% in patients below 80 years of age and 45% in patients 80 years or older.
Conclusion
Nine years of experience enabled us to exploit EVAR’s advantages as a minimally invasive method in an elective as well as emergency setting. Complications, secondary interventions and survival rates in our low volume non-university hospital matches results from larger vascular centers.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
