{"title":"单侧烟雾病所致急性硬膜下血肿合并皮质下出血后脑动脉血管合并颅成形术治疗。","authors":"Naoki Kato, Shota Kakizaki, Yusuke Hirokawa, Shotaro Michishita, Takuya Ishii, Tohru Terao, Yuichi Murayama","doi":"10.1155/2023/1787738","DOIUrl":null,"url":null,"abstract":"<p><p>Moyamoya disease is often diagnosed after intracranial hemorrhage in adult patients. Here, we report a case of unilateral moyamoya disease treated with indirect revascularization combined with cranioplasty after treatment for acute subdural hematoma and subcortical hemorrhage. A middle-aged woman with disturbed consciousness was transferred to our hospital. Computed tomography (CT) revealed an acute subdural hematoma with left temporoparietal subcortical hemorrhage. Three-dimensional CT angiography indicated a scarcely enhanced left middle cerebral artery (MCA) that was suspected to be delayed or nonfilling due to increased intracranial pressure. Subsequently, hematoma evacuation and external decompression were performed. Postoperative digital subtraction angiography (DSA) revealed stenosis of the left MCA and moyamoya vessels, indicating unilateral moyamoya disease. Forty-five days after the initial procedure, we performed encephalo-arterio-synangiosis (EAS) using the superficial temporal artery simultaneously with cranioplasty for the skull defect. The modified Rankin Scale score of the patient one year after discharge was 1, and the repeat DSA showed good patency of the EAS. Revascularization using EAS in the second step can be an option for revascularization for hemorrhagic moyamoya disease if the patient required cranioplasty for postoperative skull defect after decompressive craniotomy.</p>","PeriodicalId":9615,"journal":{"name":"Case Reports in Neurological Medicine","volume":"2023 ","pages":"1787738"},"PeriodicalIF":0.9000,"publicationDate":"2023-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9873458/pdf/","citationCount":"0","resultStr":"{\"title\":\"Encephalo-Arterio-Synangiosis with Cranioplasty after Treatment of Acute Subdural Hematoma Associated with Subcortical Hemorrhage Due to Unilateral Moyamoya Disease.\",\"authors\":\"Naoki Kato, Shota Kakizaki, Yusuke Hirokawa, Shotaro Michishita, Takuya Ishii, Tohru Terao, Yuichi Murayama\",\"doi\":\"10.1155/2023/1787738\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>Moyamoya disease is often diagnosed after intracranial hemorrhage in adult patients. Here, we report a case of unilateral moyamoya disease treated with indirect revascularization combined with cranioplasty after treatment for acute subdural hematoma and subcortical hemorrhage. A middle-aged woman with disturbed consciousness was transferred to our hospital. Computed tomography (CT) revealed an acute subdural hematoma with left temporoparietal subcortical hemorrhage. Three-dimensional CT angiography indicated a scarcely enhanced left middle cerebral artery (MCA) that was suspected to be delayed or nonfilling due to increased intracranial pressure. Subsequently, hematoma evacuation and external decompression were performed. Postoperative digital subtraction angiography (DSA) revealed stenosis of the left MCA and moyamoya vessels, indicating unilateral moyamoya disease. Forty-five days after the initial procedure, we performed encephalo-arterio-synangiosis (EAS) using the superficial temporal artery simultaneously with cranioplasty for the skull defect. The modified Rankin Scale score of the patient one year after discharge was 1, and the repeat DSA showed good patency of the EAS. Revascularization using EAS in the second step can be an option for revascularization for hemorrhagic moyamoya disease if the patient required cranioplasty for postoperative skull defect after decompressive craniotomy.</p>\",\"PeriodicalId\":9615,\"journal\":{\"name\":\"Case Reports in Neurological Medicine\",\"volume\":\"2023 \",\"pages\":\"1787738\"},\"PeriodicalIF\":0.9000,\"publicationDate\":\"2023-01-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9873458/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Case Reports in Neurological Medicine\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1155/2023/1787738\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q4\",\"JCRName\":\"CLINICAL NEUROLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Case Reports in Neurological Medicine","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1155/2023/1787738","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q4","JCRName":"CLINICAL NEUROLOGY","Score":null,"Total":0}
Encephalo-Arterio-Synangiosis with Cranioplasty after Treatment of Acute Subdural Hematoma Associated with Subcortical Hemorrhage Due to Unilateral Moyamoya Disease.
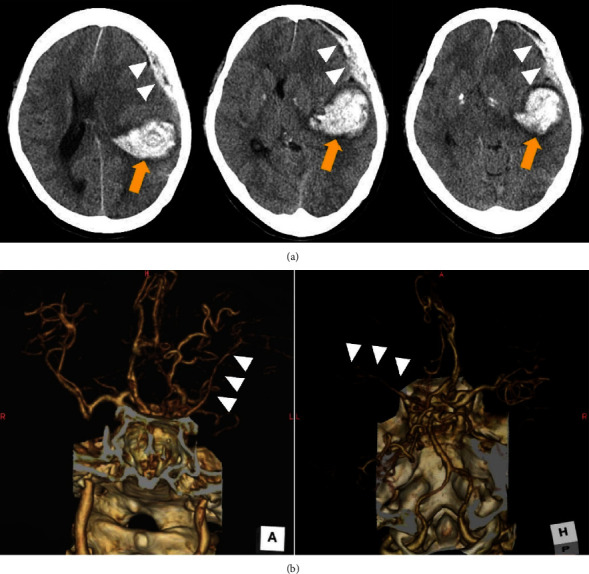
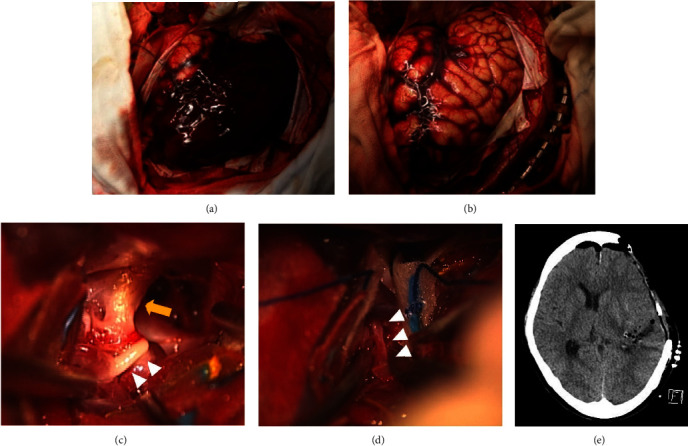
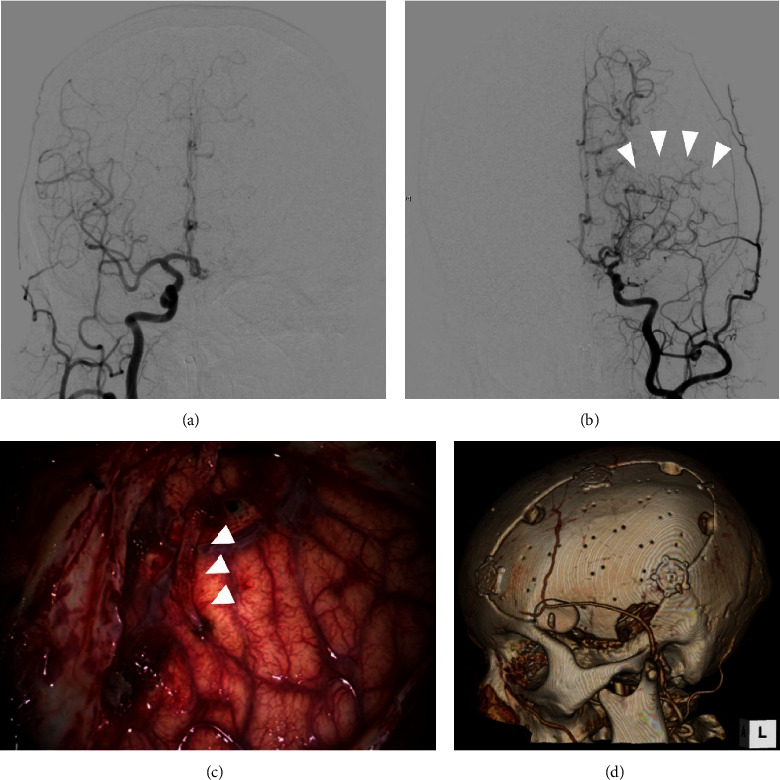
Moyamoya disease is often diagnosed after intracranial hemorrhage in adult patients. Here, we report a case of unilateral moyamoya disease treated with indirect revascularization combined with cranioplasty after treatment for acute subdural hematoma and subcortical hemorrhage. A middle-aged woman with disturbed consciousness was transferred to our hospital. Computed tomography (CT) revealed an acute subdural hematoma with left temporoparietal subcortical hemorrhage. Three-dimensional CT angiography indicated a scarcely enhanced left middle cerebral artery (MCA) that was suspected to be delayed or nonfilling due to increased intracranial pressure. Subsequently, hematoma evacuation and external decompression were performed. Postoperative digital subtraction angiography (DSA) revealed stenosis of the left MCA and moyamoya vessels, indicating unilateral moyamoya disease. Forty-five days after the initial procedure, we performed encephalo-arterio-synangiosis (EAS) using the superficial temporal artery simultaneously with cranioplasty for the skull defect. The modified Rankin Scale score of the patient one year after discharge was 1, and the repeat DSA showed good patency of the EAS. Revascularization using EAS in the second step can be an option for revascularization for hemorrhagic moyamoya disease if the patient required cranioplasty for postoperative skull defect after decompressive craniotomy.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
