Adalia H Jun-O'Connell, Shravan Sivakumar, Nils Henninger, Brian Silver, Meghna Trivedi, Mehdi Ghasemi, Rakhee R Lalla, Kimiyoshi J Kobayashi
{"title":"干预与非干预患者中风住院转院的结果。","authors":"Adalia H Jun-O'Connell, Shravan Sivakumar, Nils Henninger, Brian Silver, Meghna Trivedi, Mehdi Ghasemi, Rakhee R Lalla, Kimiyoshi J Kobayashi","doi":"10.14740/jocmr4945","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Telestroke is an established telemedicine method of delivering emergency stroke care. However, not all neurological patients utilizing telestroke service require emergency interventions or transfer to a comprehensive stroke center. To develop an understanding of the appropriateness of inter-hospital neurological transfers utilizing the telemedicine, our study aimed to assess the differences in outcomes of inter-hospital transfers utilizing the service in relation to the need for neurological interventions.</p><p><strong>Methods: </strong>The pragmatic, retrospective analysis included 181 consecutive patients, who were emergently transferred from telestroke-affiliated regional medical centers between October 3, 2021, and May 3, 2022. In this exploratory study investigating the outcomes of telestroke-referred patients, patients receiving interventions were compared to those that did not following transfer to our tertiary center. Neurological interventions included mechanical thrombectomy (MT) and/or tissue plasminogen activator (tPA), craniectomy, electroencephalography (EEG), or external ventricular drain (EVD). Transfer mortality rate, discharge functional status defined by modified Rankin scale (mRS), neurological status defined by National Institutes of Health Stroke Scale (NIHSS), 30-day unpreventable readmission rate, 90-day clinical major adverse cardiovascular events (MACE), and 90-day mRS, and NIHSS were studied. We used χ<sup>2</sup> or Fisher exact tests to evaluate the association between the intervention and categorical or dichotomous variables. Continuous or ordinal measures were compared using Wilcoxon rank-sum tests. All tests of statistical significance were considered to be significant at P < 0.05.</p><p><strong>Results: </strong>Among the 181 transferred patients, 114 (63%) received neuro-intervention and 67 (37%) did not. The death rate during the index admission was not statistically significant between the intervention and non-intervention groups (P = 0.196). The discharge NIHSS and mRS were worse in the intervention compared to the non-intervention (P < 0.05 each, respectively). The 90-day mortality and cardiovascular event rates were similar between intervention and non-intervention groups (P > 0.05 each, respectively). The 30-day readmission rates were also similar between the two groups (14% intervention vs. 13.4% non-intervention, P = 0.910). The 90-day mRS were not significantly different between intervention and non-intervention groups (median 3 (IQR: 1 - 6) vs. 2 (IQR: 0 - 6), P = 0.109). However, 90-day NIHSS was worse in the intervention compared to non-intervention group (median 2 (IQR: 0 - 11) vs. 0 (IQR: 0 - 3), P = 0.004).</p><p><strong>Conclusions: </strong>Telestroke is a valuable resource that expedites emergent neurological care via referral to a stroke center. However, not all transferred patients benefit from the transfer process. Future multicenter studies are warranted to study the effects or appropriateness of telestroke networks, and to better understand the patient characteristics, resources allocation, and transferring institutions to improve telestroke care.</p>","PeriodicalId":15431,"journal":{"name":"Journal of Clinical Medicine Research","volume":"15 6","pages":"292-299"},"PeriodicalIF":0.0000,"publicationDate":"2023-06-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/7f/c5/jocmr-15-292.PMC10332878.pdf","citationCount":"0","resultStr":"{\"title\":\"Outcomes of Telestroke Inter-Hospital Transfers Among Intervention and Non-Intervention Patients.\",\"authors\":\"Adalia H Jun-O'Connell, Shravan Sivakumar, Nils Henninger, Brian Silver, Meghna Trivedi, Mehdi Ghasemi, Rakhee R Lalla, Kimiyoshi J Kobayashi\",\"doi\":\"10.14740/jocmr4945\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Telestroke is an established telemedicine method of delivering emergency stroke care. However, not all neurological patients utilizing telestroke service require emergency interventions or transfer to a comprehensive stroke center. To develop an understanding of the appropriateness of inter-hospital neurological transfers utilizing the telemedicine, our study aimed to assess the differences in outcomes of inter-hospital transfers utilizing the service in relation to the need for neurological interventions.</p><p><strong>Methods: </strong>The pragmatic, retrospective analysis included 181 consecutive patients, who were emergently transferred from telestroke-affiliated regional medical centers between October 3, 2021, and May 3, 2022. In this exploratory study investigating the outcomes of telestroke-referred patients, patients receiving interventions were compared to those that did not following transfer to our tertiary center. Neurological interventions included mechanical thrombectomy (MT) and/or tissue plasminogen activator (tPA), craniectomy, electroencephalography (EEG), or external ventricular drain (EVD). Transfer mortality rate, discharge functional status defined by modified Rankin scale (mRS), neurological status defined by National Institutes of Health Stroke Scale (NIHSS), 30-day unpreventable readmission rate, 90-day clinical major adverse cardiovascular events (MACE), and 90-day mRS, and NIHSS were studied. We used χ<sup>2</sup> or Fisher exact tests to evaluate the association between the intervention and categorical or dichotomous variables. Continuous or ordinal measures were compared using Wilcoxon rank-sum tests. All tests of statistical significance were considered to be significant at P < 0.05.</p><p><strong>Results: </strong>Among the 181 transferred patients, 114 (63%) received neuro-intervention and 67 (37%) did not. The death rate during the index admission was not statistically significant between the intervention and non-intervention groups (P = 0.196). The discharge NIHSS and mRS were worse in the intervention compared to the non-intervention (P < 0.05 each, respectively). The 90-day mortality and cardiovascular event rates were similar between intervention and non-intervention groups (P > 0.05 each, respectively). The 30-day readmission rates were also similar between the two groups (14% intervention vs. 13.4% non-intervention, P = 0.910). The 90-day mRS were not significantly different between intervention and non-intervention groups (median 3 (IQR: 1 - 6) vs. 2 (IQR: 0 - 6), P = 0.109). However, 90-day NIHSS was worse in the intervention compared to non-intervention group (median 2 (IQR: 0 - 11) vs. 0 (IQR: 0 - 3), P = 0.004).</p><p><strong>Conclusions: </strong>Telestroke is a valuable resource that expedites emergent neurological care via referral to a stroke center. However, not all transferred patients benefit from the transfer process. Future multicenter studies are warranted to study the effects or appropriateness of telestroke networks, and to better understand the patient characteristics, resources allocation, and transferring institutions to improve telestroke care.</p>\",\"PeriodicalId\":15431,\"journal\":{\"name\":\"Journal of Clinical Medicine Research\",\"volume\":\"15 6\",\"pages\":\"292-299\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2023-06-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/7f/c5/jocmr-15-292.PMC10332878.pdf\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of Clinical Medicine Research\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.14740/jocmr4945\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Clinical Medicine Research","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.14740/jocmr4945","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
Outcomes of Telestroke Inter-Hospital Transfers Among Intervention and Non-Intervention Patients.
Background: Telestroke is an established telemedicine method of delivering emergency stroke care. However, not all neurological patients utilizing telestroke service require emergency interventions or transfer to a comprehensive stroke center. To develop an understanding of the appropriateness of inter-hospital neurological transfers utilizing the telemedicine, our study aimed to assess the differences in outcomes of inter-hospital transfers utilizing the service in relation to the need for neurological interventions.
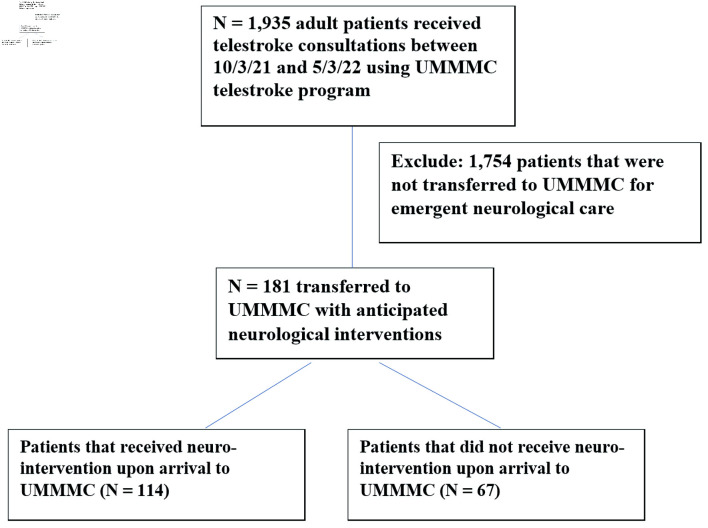
Methods: The pragmatic, retrospective analysis included 181 consecutive patients, who were emergently transferred from telestroke-affiliated regional medical centers between October 3, 2021, and May 3, 2022. In this exploratory study investigating the outcomes of telestroke-referred patients, patients receiving interventions were compared to those that did not following transfer to our tertiary center. Neurological interventions included mechanical thrombectomy (MT) and/or tissue plasminogen activator (tPA), craniectomy, electroencephalography (EEG), or external ventricular drain (EVD). Transfer mortality rate, discharge functional status defined by modified Rankin scale (mRS), neurological status defined by National Institutes of Health Stroke Scale (NIHSS), 30-day unpreventable readmission rate, 90-day clinical major adverse cardiovascular events (MACE), and 90-day mRS, and NIHSS were studied. We used χ2 or Fisher exact tests to evaluate the association between the intervention and categorical or dichotomous variables. Continuous or ordinal measures were compared using Wilcoxon rank-sum tests. All tests of statistical significance were considered to be significant at P < 0.05.
Results: Among the 181 transferred patients, 114 (63%) received neuro-intervention and 67 (37%) did not. The death rate during the index admission was not statistically significant between the intervention and non-intervention groups (P = 0.196). The discharge NIHSS and mRS were worse in the intervention compared to the non-intervention (P < 0.05 each, respectively). The 90-day mortality and cardiovascular event rates were similar between intervention and non-intervention groups (P > 0.05 each, respectively). The 30-day readmission rates were also similar between the two groups (14% intervention vs. 13.4% non-intervention, P = 0.910). The 90-day mRS were not significantly different between intervention and non-intervention groups (median 3 (IQR: 1 - 6) vs. 2 (IQR: 0 - 6), P = 0.109). However, 90-day NIHSS was worse in the intervention compared to non-intervention group (median 2 (IQR: 0 - 11) vs. 0 (IQR: 0 - 3), P = 0.004).
Conclusions: Telestroke is a valuable resource that expedites emergent neurological care via referral to a stroke center. However, not all transferred patients benefit from the transfer process. Future multicenter studies are warranted to study the effects or appropriateness of telestroke networks, and to better understand the patient characteristics, resources allocation, and transferring institutions to improve telestroke care.



 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
