{"title":"基于循环生物标志物的风险分层通过XGBoosting算法个性化急性A型主动脉夹层的弓修复策略。","authors":"Hong Liu, Si-Chong Qian, Lu Han, Ying-Yuan Zhang, Ying Wu, Liang Hong, Ji-Nong Yang, Ji-Sheng Zhong, Yu-Qi Wang, Dong-Kai Wu, Guo-Liang Fan, Jun-Quan Chen, Sheng-Qiang Zhang, Xing-Xing Peng, Zhi-Wei Tang, Al-Wajih Hamzah, Yong-Feng Shao, Hai-Yang Li, Hong-Jia Zhang","doi":"10.1093/ehjdh/ztac068","DOIUrl":null,"url":null,"abstract":"<p><strong>Aims: </strong>The incremental usefulness of circulating biomarkers from different pathological pathways for predicting mortality has not been evaluated in acute Type A aortic dissection (ATAAD) patients. We aim to develop a risk prediction model and investigate the impact of arch repair strategy on mortality based on distinct risk stratifications.</p><p><strong>Methods and results: </strong>A total of 3771 ATAAD patients who underwent aortic surgery retrospectively included were randomly divided into training and testing cohorts at a ratio of 7:3 for the development and validation of the risk model based on multiple circulating biomarkers and conventional clinical factors. Extreme gradient boosting was used to generate the risk models. Subgroup analyses were performed by risk stratifications (low vs. middle-high risk) and arch repair strategies (proximal vs. extensive arch repair). Addition of multiple biomarkers to a model with conventional factors fitted an ABC risk model consisting of platelet-leucocyte ratio, mean arterial pressure, albumin, age, creatinine, creatine kinase-MB, haemoglobin, lactate, left ventricular end-diastolic dimension, urea nitrogen, and aspartate aminotransferase, with adequate discrimination ability {area under the receiver operating characteristic curve (AUROC): 0.930 [95% confidence interval (CI) 0.906-0.954] and 0.954, 95% CI (0.930-0.977) in the derivation and validation cohort, respectively}. Compared with proximal arch repair, the extensive repair was associated with similar mortality risk among patients at low risk [odds ratio (OR) 1.838, 95% CI (0.559-6.038); <i>P</i> = 0.316], but associated with higher mortality risk among patients at middle-high risk [OR 2.007, 95% CI (1.460-2.757); <i>P</i> < 0.0001].</p><p><strong>Conclusion: </strong>In ATAAD patients, the simultaneous addition of circulating biomarkers of inflammatory, cardiac, hepatic, renal, and metabolic abnormalities substantially improved risk stratification and individualized arch repair strategy.</p>","PeriodicalId":72965,"journal":{"name":"European heart journal. Digital health","volume":"3 4","pages":"587-599"},"PeriodicalIF":3.9000,"publicationDate":"2022-12-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/70/b5/ztac068.PMC9779759.pdf","citationCount":"2","resultStr":"{\"title\":\"Circulating biomarker-based risk stratifications individualize arch repair strategy of acute Type A aortic dissection via the XGBoosting algorithm.\",\"authors\":\"Hong Liu, Si-Chong Qian, Lu Han, Ying-Yuan Zhang, Ying Wu, Liang Hong, Ji-Nong Yang, Ji-Sheng Zhong, Yu-Qi Wang, Dong-Kai Wu, Guo-Liang Fan, Jun-Quan Chen, Sheng-Qiang Zhang, Xing-Xing Peng, Zhi-Wei Tang, Al-Wajih Hamzah, Yong-Feng Shao, Hai-Yang Li, Hong-Jia Zhang\",\"doi\":\"10.1093/ehjdh/ztac068\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Aims: </strong>The incremental usefulness of circulating biomarkers from different pathological pathways for predicting mortality has not been evaluated in acute Type A aortic dissection (ATAAD) patients. We aim to develop a risk prediction model and investigate the impact of arch repair strategy on mortality based on distinct risk stratifications.</p><p><strong>Methods and results: </strong>A total of 3771 ATAAD patients who underwent aortic surgery retrospectively included were randomly divided into training and testing cohorts at a ratio of 7:3 for the development and validation of the risk model based on multiple circulating biomarkers and conventional clinical factors. Extreme gradient boosting was used to generate the risk models. Subgroup analyses were performed by risk stratifications (low vs. middle-high risk) and arch repair strategies (proximal vs. extensive arch repair). Addition of multiple biomarkers to a model with conventional factors fitted an ABC risk model consisting of platelet-leucocyte ratio, mean arterial pressure, albumin, age, creatinine, creatine kinase-MB, haemoglobin, lactate, left ventricular end-diastolic dimension, urea nitrogen, and aspartate aminotransferase, with adequate discrimination ability {area under the receiver operating characteristic curve (AUROC): 0.930 [95% confidence interval (CI) 0.906-0.954] and 0.954, 95% CI (0.930-0.977) in the derivation and validation cohort, respectively}. Compared with proximal arch repair, the extensive repair was associated with similar mortality risk among patients at low risk [odds ratio (OR) 1.838, 95% CI (0.559-6.038); <i>P</i> = 0.316], but associated with higher mortality risk among patients at middle-high risk [OR 2.007, 95% CI (1.460-2.757); <i>P</i> < 0.0001].</p><p><strong>Conclusion: </strong>In ATAAD patients, the simultaneous addition of circulating biomarkers of inflammatory, cardiac, hepatic, renal, and metabolic abnormalities substantially improved risk stratification and individualized arch repair strategy.</p>\",\"PeriodicalId\":72965,\"journal\":{\"name\":\"European heart journal. Digital health\",\"volume\":\"3 4\",\"pages\":\"587-599\"},\"PeriodicalIF\":3.9000,\"publicationDate\":\"2022-12-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/70/b5/ztac068.PMC9779759.pdf\",\"citationCount\":\"2\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"European heart journal. Digital health\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1093/ehjdh/ztac068\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"CARDIAC & CARDIOVASCULAR SYSTEMS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"European heart journal. Digital health","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1093/ehjdh/ztac068","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 2
摘要
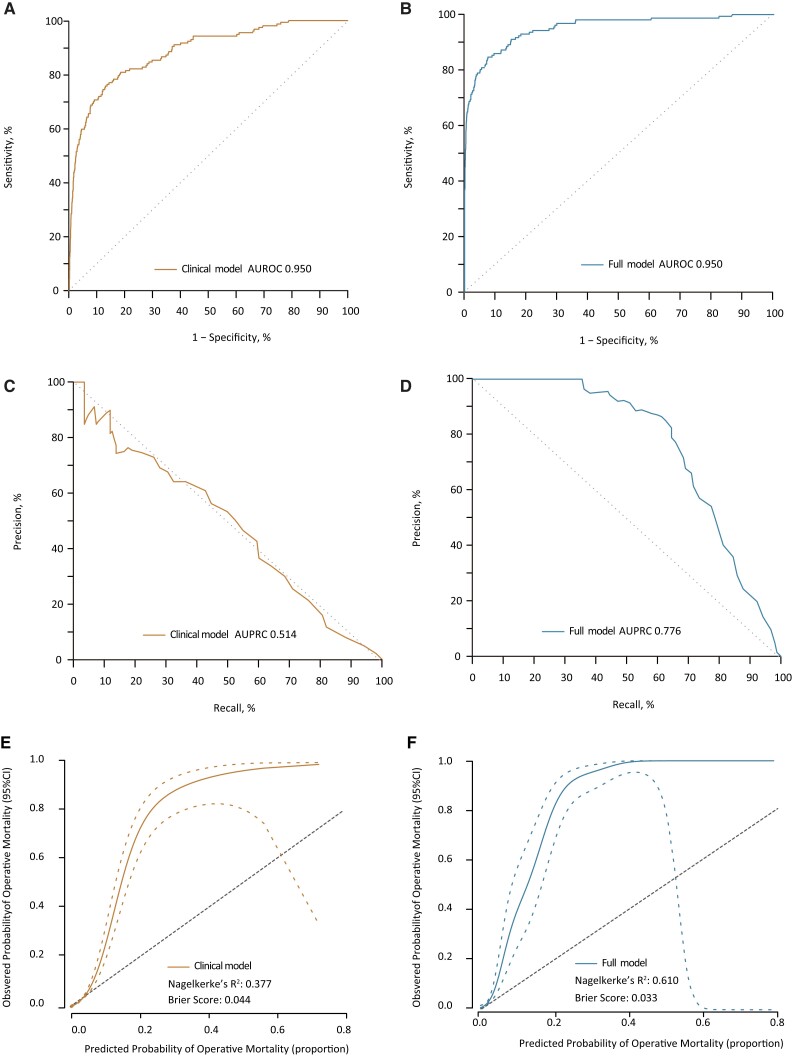
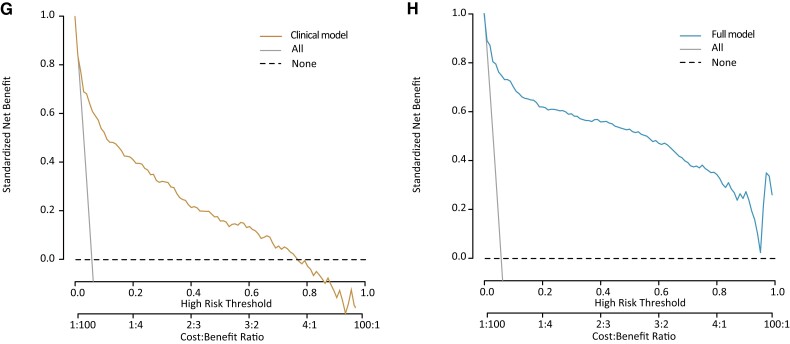
目的:在急性A型主动脉夹层(ATAAD)患者中,尚未评估不同病理途径的循环生物标志物对预测死亡率的增量有用性。我们的目标是建立一个风险预测模型,并研究基于不同风险分层的弓修复策略对死亡率的影响。方法和结果:回顾性纳入3771例接受主动脉手术的ATAAD患者,按7:3的比例随机分为训练组和测试组,以建立和验证基于多种循环生物标志物和常规临床因素的风险模型。采用极值梯度增强方法生成风险模型。根据风险分层(低风险vs中高风险)和弓修复策略(近端弓修复vs广泛弓修复)进行亚组分析。在常规因素模型中加入多种生物标志物,拟合由血小板-白细胞比、平均动脉压、白蛋白、年龄、肌酐、肌酸激酶- mb、血红蛋白、乳酸、左室舒张末期尺寸、尿素氮和天冬氨酸转氨酶组成的ABC风险模型,具有足够的识别能力{受试者工作特征曲线下面积(AUROC):0.930[95%置信区间(CI) 0.906-0.954]和0.954,95% CI(0.930-0.977)在推导和验证队列中分别}。与近端弓修复相比,低风险患者的广泛修复与相似的死亡风险相关[优势比(OR) 1.838, 95% CI (0.559-6.038);P = 0.316],但中高危患者的死亡风险较高[OR 2.007, 95% CI (1.460-2.757);P < 0.0001]。结论:在ATAAD患者中,同时添加炎症、心脏、肝脏、肾脏和代谢异常的循环生物标志物可显著改善风险分层和个体化弓修复策略。
Circulating biomarker-based risk stratifications individualize arch repair strategy of acute Type A aortic dissection via the XGBoosting algorithm.
Aims: The incremental usefulness of circulating biomarkers from different pathological pathways for predicting mortality has not been evaluated in acute Type A aortic dissection (ATAAD) patients. We aim to develop a risk prediction model and investigate the impact of arch repair strategy on mortality based on distinct risk stratifications.
Methods and results: A total of 3771 ATAAD patients who underwent aortic surgery retrospectively included were randomly divided into training and testing cohorts at a ratio of 7:3 for the development and validation of the risk model based on multiple circulating biomarkers and conventional clinical factors. Extreme gradient boosting was used to generate the risk models. Subgroup analyses were performed by risk stratifications (low vs. middle-high risk) and arch repair strategies (proximal vs. extensive arch repair). Addition of multiple biomarkers to a model with conventional factors fitted an ABC risk model consisting of platelet-leucocyte ratio, mean arterial pressure, albumin, age, creatinine, creatine kinase-MB, haemoglobin, lactate, left ventricular end-diastolic dimension, urea nitrogen, and aspartate aminotransferase, with adequate discrimination ability {area under the receiver operating characteristic curve (AUROC): 0.930 [95% confidence interval (CI) 0.906-0.954] and 0.954, 95% CI (0.930-0.977) in the derivation and validation cohort, respectively}. Compared with proximal arch repair, the extensive repair was associated with similar mortality risk among patients at low risk [odds ratio (OR) 1.838, 95% CI (0.559-6.038); P = 0.316], but associated with higher mortality risk among patients at middle-high risk [OR 2.007, 95% CI (1.460-2.757); P < 0.0001].
Conclusion: In ATAAD patients, the simultaneous addition of circulating biomarkers of inflammatory, cardiac, hepatic, renal, and metabolic abnormalities substantially improved risk stratification and individualized arch repair strategy.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
