{"title":"CAP、SSTI和UTI住院患者血液培养收集减少。","authors":"Monica D Combs, Danica B Liberman, Vivian Lee","doi":"10.1097/pq9.0000000000000705","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Blood culture collection in pediatric patients with community-acquired pneumonia (CAP), skin and soft tissue infections (SSTI), and urinary tract infections (UTI) remains high despite evidence of its limited utility. We aimed to decrease the number of cultures collected in children hospitalized for CAP, SSTI, and UTI by 25% over 11 months.</p><p><strong>Methods: </strong>Quality improvement initiative at a children's hospital among well-appearing patients aged 2 months or more to 18 years diagnosed with CAP, SSTI, or UTI. Our primary and secondary outcomes were blood culture collection rate and positivity rate, respectively. Interventions focused on three key drivers: academic detailing, physician awareness of personal performance, and data transparency.</p><p><strong>Results: </strong>Over the 2-year study period, there were 105 blood cultures collected in 223 hospitalized patients. Blood culture collection rates demonstrated special cause variation, decreasing from 63.5% to 24.5%. For patients with UTI, 86% (18/21) of blood cultures were negative, whereas 100% were negative for CAP and SSTI. All three patients with bacteremic UTI had a concurrent urine culture growing the same pathogen. Balancing measures remained unchanged, including escalation to a higher level of care and return to the emergency department or hospital within 14 days for the same infection.</p><p><strong>Conclusions: </strong>A multifaceted quality improvement approach can reduce blood culture collection for hospitalized patients with CAP, SSTI, and UTI without significant changes to balancing measures. Despite the reduction achieved, the near-universal negative culture results suggest continued overutilization and highlight the need for more targeted approaches to blood culture collection.</p>","PeriodicalId":74412,"journal":{"name":"Pediatric quality & safety","volume":"8 6","pages":"e705"},"PeriodicalIF":1.1000,"publicationDate":"2023-12-05","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10697617/pdf/","citationCount":"0","resultStr":"{\"title\":\"Decreasing Blood Culture Collection in Hospitalized Patients with CAP, SSTI, and UTI.\",\"authors\":\"Monica D Combs, Danica B Liberman, Vivian Lee\",\"doi\":\"10.1097/pq9.0000000000000705\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Blood culture collection in pediatric patients with community-acquired pneumonia (CAP), skin and soft tissue infections (SSTI), and urinary tract infections (UTI) remains high despite evidence of its limited utility. We aimed to decrease the number of cultures collected in children hospitalized for CAP, SSTI, and UTI by 25% over 11 months.</p><p><strong>Methods: </strong>Quality improvement initiative at a children's hospital among well-appearing patients aged 2 months or more to 18 years diagnosed with CAP, SSTI, or UTI. Our primary and secondary outcomes were blood culture collection rate and positivity rate, respectively. Interventions focused on three key drivers: academic detailing, physician awareness of personal performance, and data transparency.</p><p><strong>Results: </strong>Over the 2-year study period, there were 105 blood cultures collected in 223 hospitalized patients. Blood culture collection rates demonstrated special cause variation, decreasing from 63.5% to 24.5%. For patients with UTI, 86% (18/21) of blood cultures were negative, whereas 100% were negative for CAP and SSTI. All three patients with bacteremic UTI had a concurrent urine culture growing the same pathogen. Balancing measures remained unchanged, including escalation to a higher level of care and return to the emergency department or hospital within 14 days for the same infection.</p><p><strong>Conclusions: </strong>A multifaceted quality improvement approach can reduce blood culture collection for hospitalized patients with CAP, SSTI, and UTI without significant changes to balancing measures. Despite the reduction achieved, the near-universal negative culture results suggest continued overutilization and highlight the need for more targeted approaches to blood culture collection.</p>\",\"PeriodicalId\":74412,\"journal\":{\"name\":\"Pediatric quality & safety\",\"volume\":\"8 6\",\"pages\":\"e705\"},\"PeriodicalIF\":1.1000,\"publicationDate\":\"2023-12-05\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10697617/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Pediatric quality & safety\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1097/pq9.0000000000000705\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2023/11/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q3\",\"JCRName\":\"PEDIATRICS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Pediatric quality & safety","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1097/pq9.0000000000000705","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2023/11/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"PEDIATRICS","Score":null,"Total":0}
Decreasing Blood Culture Collection in Hospitalized Patients with CAP, SSTI, and UTI.
Background: Blood culture collection in pediatric patients with community-acquired pneumonia (CAP), skin and soft tissue infections (SSTI), and urinary tract infections (UTI) remains high despite evidence of its limited utility. We aimed to decrease the number of cultures collected in children hospitalized for CAP, SSTI, and UTI by 25% over 11 months.
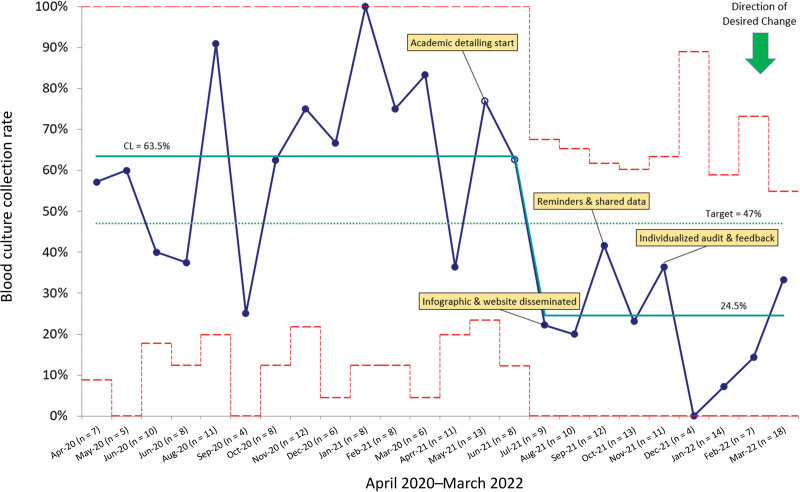
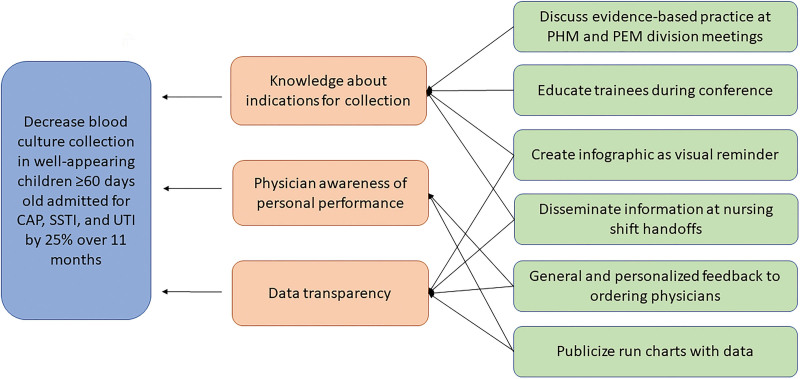
Methods: Quality improvement initiative at a children's hospital among well-appearing patients aged 2 months or more to 18 years diagnosed with CAP, SSTI, or UTI. Our primary and secondary outcomes were blood culture collection rate and positivity rate, respectively. Interventions focused on three key drivers: academic detailing, physician awareness of personal performance, and data transparency.
Results: Over the 2-year study period, there were 105 blood cultures collected in 223 hospitalized patients. Blood culture collection rates demonstrated special cause variation, decreasing from 63.5% to 24.5%. For patients with UTI, 86% (18/21) of blood cultures were negative, whereas 100% were negative for CAP and SSTI. All three patients with bacteremic UTI had a concurrent urine culture growing the same pathogen. Balancing measures remained unchanged, including escalation to a higher level of care and return to the emergency department or hospital within 14 days for the same infection.
Conclusions: A multifaceted quality improvement approach can reduce blood culture collection for hospitalized patients with CAP, SSTI, and UTI without significant changes to balancing measures. Despite the reduction achieved, the near-universal negative culture results suggest continued overutilization and highlight the need for more targeted approaches to blood culture collection.



 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
