Leonhard Mann, Felix Rosenow, Adam Strzelczyk, Elke Hattingen, Laurent M Willems, Patrick N Harter, Katharina Weber, Catrin Mann
{"title":"将耐药性局灶性癫痫患者转诊至癫痫中心进行手术前诊断的影响。","authors":"Leonhard Mann, Felix Rosenow, Adam Strzelczyk, Elke Hattingen, Laurent M Willems, Patrick N Harter, Katharina Weber, Catrin Mann","doi":"10.1186/s42466-023-00288-y","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Epilepsy surgery is an established treatment for drug-resistant focal epilepsy (DRFE) that results in seizure freedom in about 60% of patients. Correctly identifying an epileptogenic lesion in magnetic resonance imaging (MRI) is challenging but highly relevant since it improves the likelihood of being referred for presurgical diagnosis. The epileptogenic lesion's etiology directly relates to the surgical intervention's indication and outcome. Therefore, it is vital to correctly identify epileptogenic lesions and their etiology presurgically.</p><p><strong>Methods: </strong>We compared the final histopathological diagnoses of all patients with DRFE undergoing epilepsy surgery at our center between 2015 and 2021 with their MRI diagnoses before and after presurgical diagnosis at our epilepsy center, including MRI evaluations by expert epilepsy neuroradiologists. Additionally, we analyzed the outcome of different subgroups.</p><p><strong>Results: </strong>This study included 132 patients. The discordance between histopathology and MRI diagnoses significantly decreased from 61.3% for non-expert MRI evaluations (NEMRIs) to 22.1% for epilepsy center MRI evaluations (ECMRIs; p < 0.0001). The MRI-sensitivity improved significantly from 68.6% for NEMRIs to 97.7% for ECMRIs (p < 0.0001). Identifying focal cortical dysplasia (FCD) and amygdala dysplasia was the most challenging for both subgroups. 65.5% of patients with negative NEMRI were seizure-free 12 months postoperatively, no patient with negative ECMRI achieved seizure-freedom. The mean duration of epilepsy until surgical intervention was 13.6 years in patients with an initial negative NEMRI and 9.5 years in patients with a recognized lesion in NEMRI.</p><p><strong>Conclusions: </strong>This study provides evidence that for patients with DRFE-especially those with initial negative findings in a non-expert MRI-an early consultation at an epilepsy center, including an ECMRI, is important for identifying candidates for epilepsy surgery. NEMRI-negative findings preoperatively do not preclude seizure freedom postoperatively. Therefore, patients with DRFE that remain MRI-negative after initial NEMRI should be referred to an epilepsy center for presurgical evaluation. Nonreferral based on NEMRI negativity may harm such patients and delay surgical intervention. However, ECMRI-negative patients have a reduced chance of becoming seizure-free after epilepsy surgery. Further improvements in MRI technique and evaluation are needed and should be directed towards improving sensitivity for FCDs and amygdala dysplasias.</p>","PeriodicalId":94156,"journal":{"name":"Neurological research and practice","volume":"5 1","pages":"65"},"PeriodicalIF":4.0000,"publicationDate":"2023-12-14","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10720126/pdf/","citationCount":"0","resultStr":"{\"title\":\"The impact of referring patients with drug-resistant focal epilepsy to an epilepsy center for presurgical diagnosis.\",\"authors\":\"Leonhard Mann, Felix Rosenow, Adam Strzelczyk, Elke Hattingen, Laurent M Willems, Patrick N Harter, Katharina Weber, Catrin Mann\",\"doi\":\"10.1186/s42466-023-00288-y\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Epilepsy surgery is an established treatment for drug-resistant focal epilepsy (DRFE) that results in seizure freedom in about 60% of patients. Correctly identifying an epileptogenic lesion in magnetic resonance imaging (MRI) is challenging but highly relevant since it improves the likelihood of being referred for presurgical diagnosis. The epileptogenic lesion's etiology directly relates to the surgical intervention's indication and outcome. Therefore, it is vital to correctly identify epileptogenic lesions and their etiology presurgically.</p><p><strong>Methods: </strong>We compared the final histopathological diagnoses of all patients with DRFE undergoing epilepsy surgery at our center between 2015 and 2021 with their MRI diagnoses before and after presurgical diagnosis at our epilepsy center, including MRI evaluations by expert epilepsy neuroradiologists. Additionally, we analyzed the outcome of different subgroups.</p><p><strong>Results: </strong>This study included 132 patients. The discordance between histopathology and MRI diagnoses significantly decreased from 61.3% for non-expert MRI evaluations (NEMRIs) to 22.1% for epilepsy center MRI evaluations (ECMRIs; p < 0.0001). The MRI-sensitivity improved significantly from 68.6% for NEMRIs to 97.7% for ECMRIs (p < 0.0001). Identifying focal cortical dysplasia (FCD) and amygdala dysplasia was the most challenging for both subgroups. 65.5% of patients with negative NEMRI were seizure-free 12 months postoperatively, no patient with negative ECMRI achieved seizure-freedom. The mean duration of epilepsy until surgical intervention was 13.6 years in patients with an initial negative NEMRI and 9.5 years in patients with a recognized lesion in NEMRI.</p><p><strong>Conclusions: </strong>This study provides evidence that for patients with DRFE-especially those with initial negative findings in a non-expert MRI-an early consultation at an epilepsy center, including an ECMRI, is important for identifying candidates for epilepsy surgery. NEMRI-negative findings preoperatively do not preclude seizure freedom postoperatively. Therefore, patients with DRFE that remain MRI-negative after initial NEMRI should be referred to an epilepsy center for presurgical evaluation. Nonreferral based on NEMRI negativity may harm such patients and delay surgical intervention. However, ECMRI-negative patients have a reduced chance of becoming seizure-free after epilepsy surgery. Further improvements in MRI technique and evaluation are needed and should be directed towards improving sensitivity for FCDs and amygdala dysplasias.</p>\",\"PeriodicalId\":94156,\"journal\":{\"name\":\"Neurological research and practice\",\"volume\":\"5 1\",\"pages\":\"65\"},\"PeriodicalIF\":4.0000,\"publicationDate\":\"2023-12-14\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10720126/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Neurological research and practice\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1186/s42466-023-00288-y\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"Medicine\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Neurological research and practice","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1186/s42466-023-00288-y","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"Medicine","Score":null,"Total":0}
The impact of referring patients with drug-resistant focal epilepsy to an epilepsy center for presurgical diagnosis.
Background: Epilepsy surgery is an established treatment for drug-resistant focal epilepsy (DRFE) that results in seizure freedom in about 60% of patients. Correctly identifying an epileptogenic lesion in magnetic resonance imaging (MRI) is challenging but highly relevant since it improves the likelihood of being referred for presurgical diagnosis. The epileptogenic lesion's etiology directly relates to the surgical intervention's indication and outcome. Therefore, it is vital to correctly identify epileptogenic lesions and their etiology presurgically.
Methods: We compared the final histopathological diagnoses of all patients with DRFE undergoing epilepsy surgery at our center between 2015 and 2021 with their MRI diagnoses before and after presurgical diagnosis at our epilepsy center, including MRI evaluations by expert epilepsy neuroradiologists. Additionally, we analyzed the outcome of different subgroups.
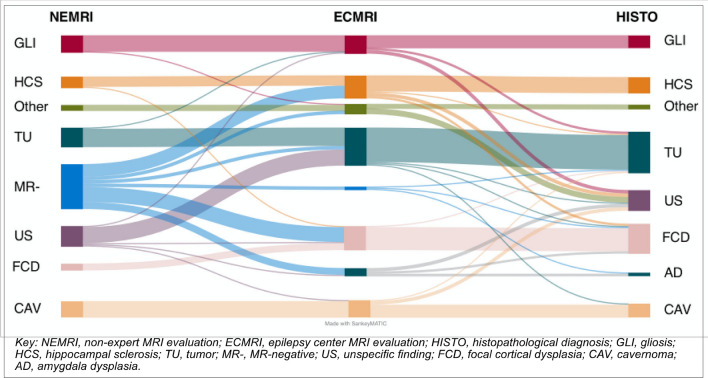
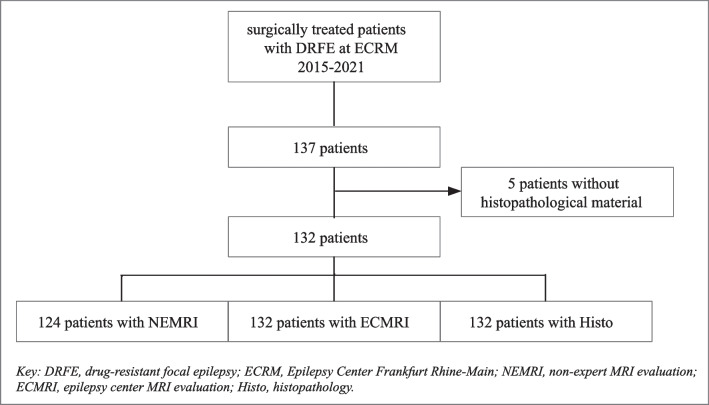
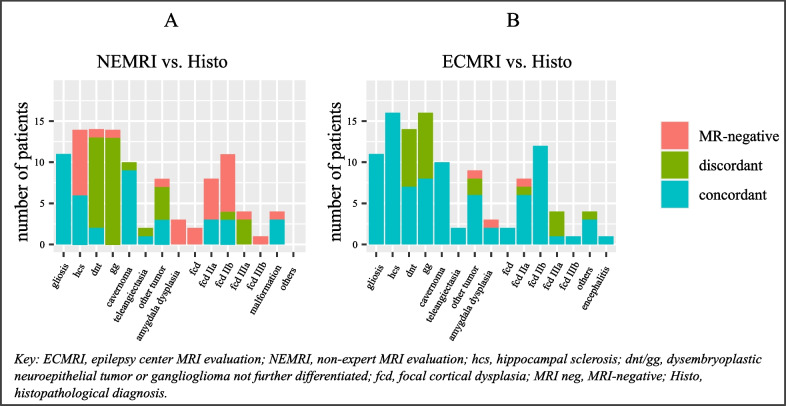
Results: This study included 132 patients. The discordance between histopathology and MRI diagnoses significantly decreased from 61.3% for non-expert MRI evaluations (NEMRIs) to 22.1% for epilepsy center MRI evaluations (ECMRIs; p < 0.0001). The MRI-sensitivity improved significantly from 68.6% for NEMRIs to 97.7% for ECMRIs (p < 0.0001). Identifying focal cortical dysplasia (FCD) and amygdala dysplasia was the most challenging for both subgroups. 65.5% of patients with negative NEMRI were seizure-free 12 months postoperatively, no patient with negative ECMRI achieved seizure-freedom. The mean duration of epilepsy until surgical intervention was 13.6 years in patients with an initial negative NEMRI and 9.5 years in patients with a recognized lesion in NEMRI.
Conclusions: This study provides evidence that for patients with DRFE-especially those with initial negative findings in a non-expert MRI-an early consultation at an epilepsy center, including an ECMRI, is important for identifying candidates for epilepsy surgery. NEMRI-negative findings preoperatively do not preclude seizure freedom postoperatively. Therefore, patients with DRFE that remain MRI-negative after initial NEMRI should be referred to an epilepsy center for presurgical evaluation. Nonreferral based on NEMRI negativity may harm such patients and delay surgical intervention. However, ECMRI-negative patients have a reduced chance of becoming seizure-free after epilepsy surgery. Further improvements in MRI technique and evaluation are needed and should be directed towards improving sensitivity for FCDs and amygdala dysplasias.



 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
