{"title":"古普塔评分对非心脏非血管手术术前心脏病学会诊请求的影响。","authors":"Funda Atar, Fatma Özkan Sipahioğlu, Gülsen Keskin, Aslı Dönmez","doi":"10.4274/TJAR.2023.231464","DOIUrl":null,"url":null,"abstract":"<p><strong>Objective: </strong>Cardiologists are the most frequently consulted specialists during pre-operative evaluations. However, unnecessary cardiology consultations (CC) can increase cardiologists' workload without impacting anaesthesia practice, resulting in delayed surgeries and additional financial burdens. We hypothesize that using Gupta during the preoperative period can reduce these adverse effects.</p><p><strong>Methods: </strong>This prospective study included patients scheduled for elective noncardiac, nonvascular surgeries who underwent pre-operative assessment. Patients who had no specific risk index used for preoperative cardiac risk evaluation were classified as Group I, and those evaluated using the Gupta scale were classified as Group II. The study compared preoperative CC, diagnostic tests, surgical delays, major adverse cardiac event (MACE), length of hospital stay and intensive care unit (ICU) stay, mortality, and costs.</p><p><strong>Results: </strong>A total of 898 patients were included in the study, with 487 in Group I and 411 in Group II. The Gupta group reduced the demand for preoperative CC (P<0.001) and preoperative non-invasive diagnostic testing (n = 107, 21.9% vs. n = 36, 8.75%). The time from the anaesthesiology outpatient clinic to surgery was 15 days in Group I and 14 days in Group II (<i>P</i>=0.132). The length of ICU stay was higher in Group I (<i>P</i>=0.019). MACE was 15 patients (3.08%) in Group I and 9 patients (2.19%) in Group II (<i>P</i>=0.076). The cost of patients in Group I was higher than that in Group II (<i>P</i>=0.019).</p><p><strong>Conclusion: </strong>Using Gupta in preoperative evaluation may reduce unnecessary preoperative resource usage, surgical delays, ICU hospitalization rates, additional costs, and mortality.</p>","PeriodicalId":23353,"journal":{"name":"Turkish journal of anaesthesiology and reanimation","volume":"51 6","pages":"485-490"},"PeriodicalIF":0.9000,"publicationDate":"2023-12-27","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10758665/pdf/","citationCount":"0","resultStr":"{\"title\":\"Effect of the Gupta Score on Pre-operative Cardiology Consultation Requests in Noncardiac Nonvascular Surgery.\",\"authors\":\"Funda Atar, Fatma Özkan Sipahioğlu, Gülsen Keskin, Aslı Dönmez\",\"doi\":\"10.4274/TJAR.2023.231464\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Objective: </strong>Cardiologists are the most frequently consulted specialists during pre-operative evaluations. However, unnecessary cardiology consultations (CC) can increase cardiologists' workload without impacting anaesthesia practice, resulting in delayed surgeries and additional financial burdens. We hypothesize that using Gupta during the preoperative period can reduce these adverse effects.</p><p><strong>Methods: </strong>This prospective study included patients scheduled for elective noncardiac, nonvascular surgeries who underwent pre-operative assessment. Patients who had no specific risk index used for preoperative cardiac risk evaluation were classified as Group I, and those evaluated using the Gupta scale were classified as Group II. The study compared preoperative CC, diagnostic tests, surgical delays, major adverse cardiac event (MACE), length of hospital stay and intensive care unit (ICU) stay, mortality, and costs.</p><p><strong>Results: </strong>A total of 898 patients were included in the study, with 487 in Group I and 411 in Group II. The Gupta group reduced the demand for preoperative CC (P<0.001) and preoperative non-invasive diagnostic testing (n = 107, 21.9% vs. n = 36, 8.75%). The time from the anaesthesiology outpatient clinic to surgery was 15 days in Group I and 14 days in Group II (<i>P</i>=0.132). The length of ICU stay was higher in Group I (<i>P</i>=0.019). MACE was 15 patients (3.08%) in Group I and 9 patients (2.19%) in Group II (<i>P</i>=0.076). The cost of patients in Group I was higher than that in Group II (<i>P</i>=0.019).</p><p><strong>Conclusion: </strong>Using Gupta in preoperative evaluation may reduce unnecessary preoperative resource usage, surgical delays, ICU hospitalization rates, additional costs, and mortality.</p>\",\"PeriodicalId\":23353,\"journal\":{\"name\":\"Turkish journal of anaesthesiology and reanimation\",\"volume\":\"51 6\",\"pages\":\"485-490\"},\"PeriodicalIF\":0.9000,\"publicationDate\":\"2023-12-27\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10758665/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Turkish journal of anaesthesiology and reanimation\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.4274/TJAR.2023.231464\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q3\",\"JCRName\":\"ANESTHESIOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Turkish journal of anaesthesiology and reanimation","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.4274/TJAR.2023.231464","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"ANESTHESIOLOGY","Score":null,"Total":0}
引用次数: 0
摘要
目的:心脏病专家是术前评估中最常咨询的专家。然而,不必要的心脏科会诊(CC)会在不影响麻醉实践的情况下增加心脏科医生的工作量,导致手术延迟和额外的经济负担。我们假设在术前使用 Gupta 可以减少这些不利影响:这项前瞻性研究纳入了接受术前评估的择期非心脏、非血管手术患者。术前心脏风险评估未使用特定风险指数的患者被分为 I 组,使用古普塔量表进行评估的患者被分为 II 组。研究比较了术前CC、诊断测试、手术延迟、主要心脏不良事件(MACE)、住院时间和重症监护室(ICU)停留时间、死亡率和费用:研究共纳入 898 名患者,其中第一组 487 人,第二组 411 人。Gupta组减少了术前CC的需求量(PP=0.132)。第一组的重症监护室住院时间较长(P=0.019)。MACE 在 I 组为 15 例(3.08%),II 组为 9 例(2.19%)(P=0.076)。第一组患者的费用高于第二组(P=0.019):结论:在术前评估中使用 Gupta 可以减少不必要的术前资源使用、手术延迟、ICU 住院率、额外费用和死亡率。
Effect of the Gupta Score on Pre-operative Cardiology Consultation Requests in Noncardiac Nonvascular Surgery.
Objective: Cardiologists are the most frequently consulted specialists during pre-operative evaluations. However, unnecessary cardiology consultations (CC) can increase cardiologists' workload without impacting anaesthesia practice, resulting in delayed surgeries and additional financial burdens. We hypothesize that using Gupta during the preoperative period can reduce these adverse effects.
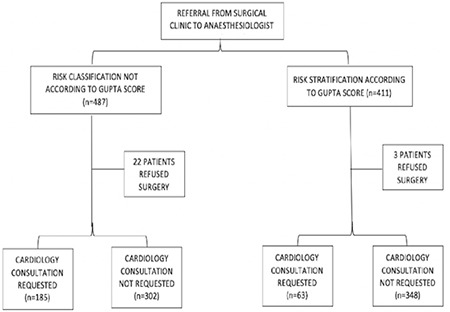
Methods: This prospective study included patients scheduled for elective noncardiac, nonvascular surgeries who underwent pre-operative assessment. Patients who had no specific risk index used for preoperative cardiac risk evaluation were classified as Group I, and those evaluated using the Gupta scale were classified as Group II. The study compared preoperative CC, diagnostic tests, surgical delays, major adverse cardiac event (MACE), length of hospital stay and intensive care unit (ICU) stay, mortality, and costs.
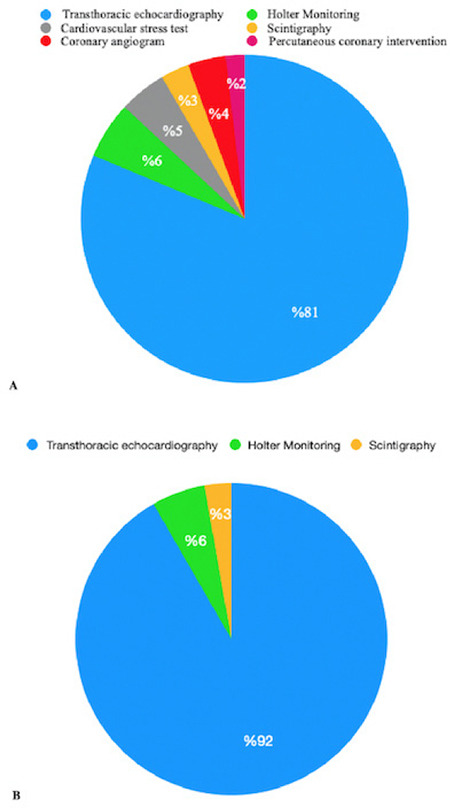
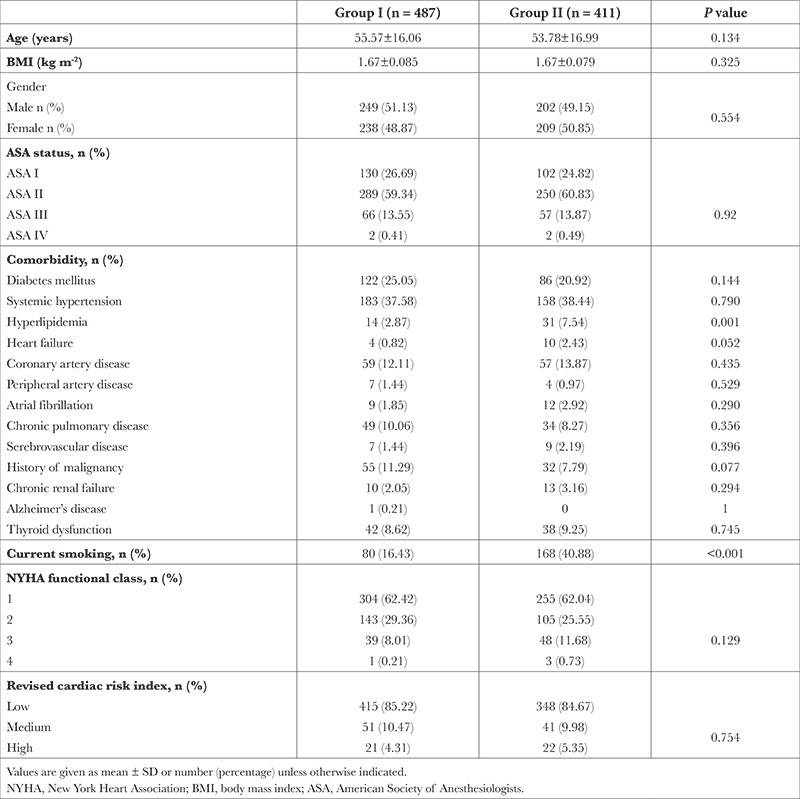
Results: A total of 898 patients were included in the study, with 487 in Group I and 411 in Group II. The Gupta group reduced the demand for preoperative CC (P<0.001) and preoperative non-invasive diagnostic testing (n = 107, 21.9% vs. n = 36, 8.75%). The time from the anaesthesiology outpatient clinic to surgery was 15 days in Group I and 14 days in Group II (P=0.132). The length of ICU stay was higher in Group I (P=0.019). MACE was 15 patients (3.08%) in Group I and 9 patients (2.19%) in Group II (P=0.076). The cost of patients in Group I was higher than that in Group II (P=0.019).
Conclusion: Using Gupta in preoperative evaluation may reduce unnecessary preoperative resource usage, surgical delays, ICU hospitalization rates, additional costs, and mortality.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
