Joseph Piscitelli, Micaela B Reddy, Lance Wollenberg, Laurence Del Frari, Jason Gong, Linda Wood, Yizhong Zhang, Kyle Matschke, Jason H Williams
{"title":"安可拉非尼对布洛芬、瑞舒伐他汀和铜卟啉 I 影响的临床评估以及他汀类药物联合用药的注意事项。","authors":"Joseph Piscitelli, Micaela B Reddy, Lance Wollenberg, Laurence Del Frari, Jason Gong, Linda Wood, Yizhong Zhang, Kyle Matschke, Jason H Williams","doi":"10.1007/s40262-024-01352-9","DOIUrl":null,"url":null,"abstract":"<p><strong>Background and objectives: </strong>Encorafenib is a kinase inhibitor indicated for the treatment of patients with unresectable or metastatic melanoma or metastatic colorectal cancer, respectively, with selected BRAF V600 mutations. A clinical drug-drug interaction (DDI) study was designed to evaluate the effect of encorafenib on rosuvastatin, a sensitive substrate of OATP1B1/3 and breast cancer resistance protein (BCRP), and bupropion, a sensitive CYP2B6 substrate. Coproporphyrin I (CP-I), an endogenous substrate for OATP1B1, was measured in a separate study to deconvolute the mechanism of transporter DDI.</p><p><strong>Methods: </strong>DDI study participants received a single oral dose of rosuvastatin (10 mg) and bupropion (75 mg) on days - 7, 1, and 14 and continuous doses of encorafenib (450 mg QD) and binimetinib (45 mg BID) starting on day 1. The CP-I data were collected from participants in a phase 3 study who received encorafenib (300 mg QD) and cetuximab (400 mg/m<sup>2</sup> initial dose, then 250 mg/m<sup>2</sup> QW). Pharmacokinetic and pharmacodynamic analysis was performed using noncompartmental and compartmental methods.</p><p><strong>Results: </strong>Bupropion exposure was not increased, whereas rosuvastatin C<sub>max</sub> and area under the receiver operating characteristic curve (AUC) increased approximately 2.7 and 1.6-fold, respectively, following repeated doses of encorafenib and binimetinib. Increase in CP-I was minimal, suggesting that the primary effect of encorafenib on rosuvastatin is through BCRP. Categorization of statins on the basis of their metabolic and transporter profile suggests pravastatin would have the least potential for interaction when coadministered with encorafenib.</p><p><strong>Conclusion: </strong>The results from these clinical studies suggest that encorafenib does not cause clinically relevant CYP2B6 induction or inhibition but is an inhibitor of BCRP and may also inhibit OATP1B1/3 to a lesser extent. Based on these results, it may be necessary to consider switching statins or reducing statin dosage accordingly for coadministration with encorafenib.</p><p><strong>Clinical trial registration: </strong>ClinicalTrials.gov NCT03864042, registered 6 March 2019.</p>","PeriodicalId":10405,"journal":{"name":"Clinical Pharmacokinetics","volume":" ","pages":"483-496"},"PeriodicalIF":4.0000,"publicationDate":"2024-04-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11052825/pdf/","citationCount":"0","resultStr":"{\"title\":\"Clinical Evaluation of the Effect of Encorafenib on Bupropion, Rosuvastatin, and Coproporphyrin I and Considerations for Statin Coadministration.\",\"authors\":\"Joseph Piscitelli, Micaela B Reddy, Lance Wollenberg, Laurence Del Frari, Jason Gong, Linda Wood, Yizhong Zhang, Kyle Matschke, Jason H Williams\",\"doi\":\"10.1007/s40262-024-01352-9\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background and objectives: </strong>Encorafenib is a kinase inhibitor indicated for the treatment of patients with unresectable or metastatic melanoma or metastatic colorectal cancer, respectively, with selected BRAF V600 mutations. A clinical drug-drug interaction (DDI) study was designed to evaluate the effect of encorafenib on rosuvastatin, a sensitive substrate of OATP1B1/3 and breast cancer resistance protein (BCRP), and bupropion, a sensitive CYP2B6 substrate. Coproporphyrin I (CP-I), an endogenous substrate for OATP1B1, was measured in a separate study to deconvolute the mechanism of transporter DDI.</p><p><strong>Methods: </strong>DDI study participants received a single oral dose of rosuvastatin (10 mg) and bupropion (75 mg) on days - 7, 1, and 14 and continuous doses of encorafenib (450 mg QD) and binimetinib (45 mg BID) starting on day 1. The CP-I data were collected from participants in a phase 3 study who received encorafenib (300 mg QD) and cetuximab (400 mg/m<sup>2</sup> initial dose, then 250 mg/m<sup>2</sup> QW). Pharmacokinetic and pharmacodynamic analysis was performed using noncompartmental and compartmental methods.</p><p><strong>Results: </strong>Bupropion exposure was not increased, whereas rosuvastatin C<sub>max</sub> and area under the receiver operating characteristic curve (AUC) increased approximately 2.7 and 1.6-fold, respectively, following repeated doses of encorafenib and binimetinib. Increase in CP-I was minimal, suggesting that the primary effect of encorafenib on rosuvastatin is through BCRP. Categorization of statins on the basis of their metabolic and transporter profile suggests pravastatin would have the least potential for interaction when coadministered with encorafenib.</p><p><strong>Conclusion: </strong>The results from these clinical studies suggest that encorafenib does not cause clinically relevant CYP2B6 induction or inhibition but is an inhibitor of BCRP and may also inhibit OATP1B1/3 to a lesser extent. Based on these results, it may be necessary to consider switching statins or reducing statin dosage accordingly for coadministration with encorafenib.</p><p><strong>Clinical trial registration: </strong>ClinicalTrials.gov NCT03864042, registered 6 March 2019.</p>\",\"PeriodicalId\":10405,\"journal\":{\"name\":\"Clinical Pharmacokinetics\",\"volume\":\" \",\"pages\":\"483-496\"},\"PeriodicalIF\":4.0000,\"publicationDate\":\"2024-04-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11052825/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Clinical Pharmacokinetics\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1007/s40262-024-01352-9\",\"RegionNum\":2,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/2/29 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q1\",\"JCRName\":\"PHARMACOLOGY & PHARMACY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Clinical Pharmacokinetics","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1007/s40262-024-01352-9","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/2/29 0:00:00","PubModel":"Epub","JCR":"Q1","JCRName":"PHARMACOLOGY & PHARMACY","Score":null,"Total":0}
Clinical Evaluation of the Effect of Encorafenib on Bupropion, Rosuvastatin, and Coproporphyrin I and Considerations for Statin Coadministration.
Background and objectives: Encorafenib is a kinase inhibitor indicated for the treatment of patients with unresectable or metastatic melanoma or metastatic colorectal cancer, respectively, with selected BRAF V600 mutations. A clinical drug-drug interaction (DDI) study was designed to evaluate the effect of encorafenib on rosuvastatin, a sensitive substrate of OATP1B1/3 and breast cancer resistance protein (BCRP), and bupropion, a sensitive CYP2B6 substrate. Coproporphyrin I (CP-I), an endogenous substrate for OATP1B1, was measured in a separate study to deconvolute the mechanism of transporter DDI.
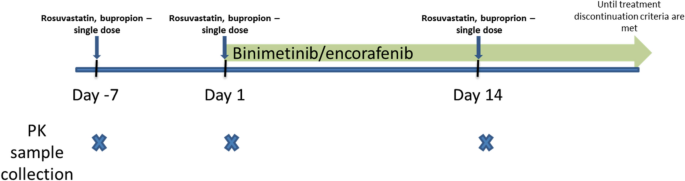
Methods: DDI study participants received a single oral dose of rosuvastatin (10 mg) and bupropion (75 mg) on days - 7, 1, and 14 and continuous doses of encorafenib (450 mg QD) and binimetinib (45 mg BID) starting on day 1. The CP-I data were collected from participants in a phase 3 study who received encorafenib (300 mg QD) and cetuximab (400 mg/m2 initial dose, then 250 mg/m2 QW). Pharmacokinetic and pharmacodynamic analysis was performed using noncompartmental and compartmental methods.
Results: Bupropion exposure was not increased, whereas rosuvastatin Cmax and area under the receiver operating characteristic curve (AUC) increased approximately 2.7 and 1.6-fold, respectively, following repeated doses of encorafenib and binimetinib. Increase in CP-I was minimal, suggesting that the primary effect of encorafenib on rosuvastatin is through BCRP. Categorization of statins on the basis of their metabolic and transporter profile suggests pravastatin would have the least potential for interaction when coadministered with encorafenib.
Conclusion: The results from these clinical studies suggest that encorafenib does not cause clinically relevant CYP2B6 induction or inhibition but is an inhibitor of BCRP and may also inhibit OATP1B1/3 to a lesser extent. Based on these results, it may be necessary to consider switching statins or reducing statin dosage accordingly for coadministration with encorafenib.
Clinical trial registration: ClinicalTrials.gov NCT03864042, registered 6 March 2019.
期刊介绍:
Clinical Pharmacokinetics promotes the continuing development of clinical pharmacokinetics and pharmacodynamics for the improvement of drug therapy, and for furthering postgraduate education in clinical pharmacology and therapeutics.
Pharmacokinetics, the study of drug disposition in the body, is an integral part of drug development and rational use. Knowledge and application of pharmacokinetic principles leads to accelerated drug development, cost effective drug use and a reduced frequency of adverse effects and drug interactions.



 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
