Matej Jenko, Katarina Mencin, Vesna Novak-Jankovic, Alenka Spindler-Vesel
{"title":"不同术中液体管理对腹部肿瘤切除术后效果的影响。","authors":"Matej Jenko, Katarina Mencin, Vesna Novak-Jankovic, Alenka Spindler-Vesel","doi":"10.2478/raon-2024-0015","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Intraoperative fluid management is a crucial aspect of cancer surgery, including colorectal surgery and pancreatoduodenectomy. The study tests if intraoperative multimodal monitoring reduces postoperative morbidity and duration of hospitalisation in patients undergoing major abdominal surgery treated by the same anaesthetic protocols with epidural analgesia.</p><p><strong>Patients and methods: </strong>A prospective study was conducted in 2 parallel groups. High-risk surgical patients undergoing major abdominal surgery were randomly selected in the control group (CG), where standard monitoring was applied (44 patients), and the protocol group (PG), where cerebral oxygenation and extended hemodynamic monitoring were used with the protocol for intraoperative interventions (44 patients).</p><p><strong>Results: </strong>There were no differences in the median length of hospital stay, CG 9 days (interquartile range [IQR] 8 days), PG 9 (5.5), p = 0.851. There was no difference in postoperative renal of cardiac impairment. Procalcitonin was significantly higher (highest postoperative value in the first 3 days) in CG, 0.75 mcg/L (IQR 3.19 mcg/L), than in PG, 0.3 mcg/L (0.88 mcg/L), p = 0.001. PG patients received a larger volume of intraoperative fluid; median intraoperative fluid balance +1300 ml (IQR 1063 ml) than CG; +375 ml (IQR 438 ml), p < 0.001.</p><p><strong>Conclusions: </strong>There were significant differences in intraoperative fluid management and vasopressor use. The median postoperative value of procalcitonin was significantly higher in CG, suggesting differences in immune response to tissue trauma in different intraoperative fluid status, but there was no difference in postoperative morbidity or hospital stay.</p>","PeriodicalId":21034,"journal":{"name":"Radiology and Oncology","volume":" ","pages":"279-288"},"PeriodicalIF":2.2000,"publicationDate":"2024-03-07","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11165984/pdf/","citationCount":"0","resultStr":"{\"title\":\"Influence of different intraoperative fluid management on postoperative outcome after abdominal tumours resection.\",\"authors\":\"Matej Jenko, Katarina Mencin, Vesna Novak-Jankovic, Alenka Spindler-Vesel\",\"doi\":\"10.2478/raon-2024-0015\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Intraoperative fluid management is a crucial aspect of cancer surgery, including colorectal surgery and pancreatoduodenectomy. The study tests if intraoperative multimodal monitoring reduces postoperative morbidity and duration of hospitalisation in patients undergoing major abdominal surgery treated by the same anaesthetic protocols with epidural analgesia.</p><p><strong>Patients and methods: </strong>A prospective study was conducted in 2 parallel groups. High-risk surgical patients undergoing major abdominal surgery were randomly selected in the control group (CG), where standard monitoring was applied (44 patients), and the protocol group (PG), where cerebral oxygenation and extended hemodynamic monitoring were used with the protocol for intraoperative interventions (44 patients).</p><p><strong>Results: </strong>There were no differences in the median length of hospital stay, CG 9 days (interquartile range [IQR] 8 days), PG 9 (5.5), p = 0.851. There was no difference in postoperative renal of cardiac impairment. Procalcitonin was significantly higher (highest postoperative value in the first 3 days) in CG, 0.75 mcg/L (IQR 3.19 mcg/L), than in PG, 0.3 mcg/L (0.88 mcg/L), p = 0.001. PG patients received a larger volume of intraoperative fluid; median intraoperative fluid balance +1300 ml (IQR 1063 ml) than CG; +375 ml (IQR 438 ml), p < 0.001.</p><p><strong>Conclusions: </strong>There were significant differences in intraoperative fluid management and vasopressor use. The median postoperative value of procalcitonin was significantly higher in CG, suggesting differences in immune response to tissue trauma in different intraoperative fluid status, but there was no difference in postoperative morbidity or hospital stay.</p>\",\"PeriodicalId\":21034,\"journal\":{\"name\":\"Radiology and Oncology\",\"volume\":\" \",\"pages\":\"279-288\"},\"PeriodicalIF\":2.2000,\"publicationDate\":\"2024-03-07\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11165984/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Radiology and Oncology\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.2478/raon-2024-0015\",\"RegionNum\":4,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/6/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q3\",\"JCRName\":\"ONCOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Radiology and Oncology","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.2478/raon-2024-0015","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/6/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"ONCOLOGY","Score":null,"Total":0}
Influence of different intraoperative fluid management on postoperative outcome after abdominal tumours resection.
Background: Intraoperative fluid management is a crucial aspect of cancer surgery, including colorectal surgery and pancreatoduodenectomy. The study tests if intraoperative multimodal monitoring reduces postoperative morbidity and duration of hospitalisation in patients undergoing major abdominal surgery treated by the same anaesthetic protocols with epidural analgesia.
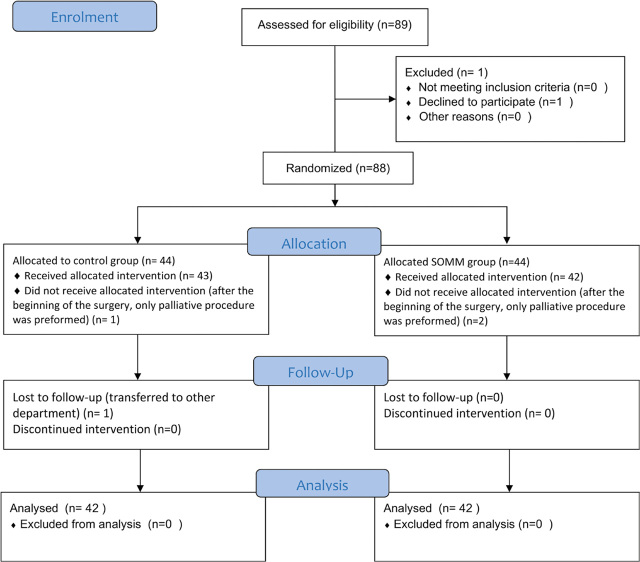
Patients and methods: A prospective study was conducted in 2 parallel groups. High-risk surgical patients undergoing major abdominal surgery were randomly selected in the control group (CG), where standard monitoring was applied (44 patients), and the protocol group (PG), where cerebral oxygenation and extended hemodynamic monitoring were used with the protocol for intraoperative interventions (44 patients).
Results: There were no differences in the median length of hospital stay, CG 9 days (interquartile range [IQR] 8 days), PG 9 (5.5), p = 0.851. There was no difference in postoperative renal of cardiac impairment. Procalcitonin was significantly higher (highest postoperative value in the first 3 days) in CG, 0.75 mcg/L (IQR 3.19 mcg/L), than in PG, 0.3 mcg/L (0.88 mcg/L), p = 0.001. PG patients received a larger volume of intraoperative fluid; median intraoperative fluid balance +1300 ml (IQR 1063 ml) than CG; +375 ml (IQR 438 ml), p < 0.001.
Conclusions: There were significant differences in intraoperative fluid management and vasopressor use. The median postoperative value of procalcitonin was significantly higher in CG, suggesting differences in immune response to tissue trauma in different intraoperative fluid status, but there was no difference in postoperative morbidity or hospital stay.
期刊介绍:
Radiology and Oncology is a multidisciplinary journal devoted to the publishing original and high quality scientific papers and review articles, pertinent to diagnostic and interventional radiology, computerized tomography, magnetic resonance, ultrasound, nuclear medicine, radiotherapy, clinical and experimental oncology, radiobiology, medical physics and radiation protection. Therefore, the scope of the journal is to cover beside radiology the diagnostic and therapeutic aspects in oncology, which distinguishes it from other journals in the field.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
