Wesley Rajaleelan, Eugene Tuyishime, Eric Plitman, Zoe Unger, Lakshmi Venkataraghavan, Michael Dinsmore
{"title":"俯卧位紧急气道管理:基于人体模型的观察性模拟研究。","authors":"Wesley Rajaleelan, Eugene Tuyishime, Eric Plitman, Zoe Unger, Lakshmi Venkataraghavan, Michael Dinsmore","doi":"10.1186/s41077-024-00285-4","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Accidental extubation during prone position can be a life-threatening emergency requiring rapid establishment of the airway. However, there is limited evidence of the best airway rescue method for this potentially catastrophic emergency. The aim of this study was to determine the most effective method to recover the airway in case of accidental extubation during prone positioning by comparing three techniques (supraglottic airway, video laryngoscopy, and fiber-optic bronchoscopy) in a simulated environment.</p><p><strong>Methods: </strong>Eleven anesthesiologists and 12 anesthesia fellows performed the simulated airway management using 3 different techniques on a mannequin positioned prone in head pins. Time required for definitive airway management and the success rates were measured.</p><p><strong>Results: </strong>The success rates of airway rescue were 100% with the supraglottic airway device (SAD), 69.6% with the video laryngoscope (CMAC), and 91.3% with the FOB. The mean (SD) time to insertion was 18.1 (4.8) s for the supraglottic airway, 78.3 (32.0) s for the CMAC, and 57.3 (24.6) s for the FOB. There were significant differences in the time required for definitive airway management between the SAD and FOB (t = 5.79, p < 0.001, 95% CI = 25.92-52.38), the SAD and CMAC (t = 8.90, p < 0.001, 95% CI = 46.93-73.40), and the FOB and CMAC (t = 3.11, p = 0.003, 95% CI = 7.78-34.25).</p><p><strong>Conclusion: </strong>The results of this simulation-based study suggest that the SAD I-gel is the best technique to manage accidental extubation during prone position by establishing a temporary airway with excellent success rate and shorter procedure time. When comparing techniques for securing a definitive airway, the FOB was more successful than the CMAC.</p>","PeriodicalId":72108,"journal":{"name":"Advances in simulation (London, England)","volume":"9 1","pages":"14"},"PeriodicalIF":4.7000,"publicationDate":"2024-04-06","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10998376/pdf/","citationCount":"0","resultStr":"{\"title\":\"Emergency airway management in the prone position: an observational mannequin-based simulation study.\",\"authors\":\"Wesley Rajaleelan, Eugene Tuyishime, Eric Plitman, Zoe Unger, Lakshmi Venkataraghavan, Michael Dinsmore\",\"doi\":\"10.1186/s41077-024-00285-4\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Introduction: </strong>Accidental extubation during prone position can be a life-threatening emergency requiring rapid establishment of the airway. However, there is limited evidence of the best airway rescue method for this potentially catastrophic emergency. The aim of this study was to determine the most effective method to recover the airway in case of accidental extubation during prone positioning by comparing three techniques (supraglottic airway, video laryngoscopy, and fiber-optic bronchoscopy) in a simulated environment.</p><p><strong>Methods: </strong>Eleven anesthesiologists and 12 anesthesia fellows performed the simulated airway management using 3 different techniques on a mannequin positioned prone in head pins. Time required for definitive airway management and the success rates were measured.</p><p><strong>Results: </strong>The success rates of airway rescue were 100% with the supraglottic airway device (SAD), 69.6% with the video laryngoscope (CMAC), and 91.3% with the FOB. The mean (SD) time to insertion was 18.1 (4.8) s for the supraglottic airway, 78.3 (32.0) s for the CMAC, and 57.3 (24.6) s for the FOB. There were significant differences in the time required for definitive airway management between the SAD and FOB (t = 5.79, p < 0.001, 95% CI = 25.92-52.38), the SAD and CMAC (t = 8.90, p < 0.001, 95% CI = 46.93-73.40), and the FOB and CMAC (t = 3.11, p = 0.003, 95% CI = 7.78-34.25).</p><p><strong>Conclusion: </strong>The results of this simulation-based study suggest that the SAD I-gel is the best technique to manage accidental extubation during prone position by establishing a temporary airway with excellent success rate and shorter procedure time. When comparing techniques for securing a definitive airway, the FOB was more successful than the CMAC.</p>\",\"PeriodicalId\":72108,\"journal\":{\"name\":\"Advances in simulation (London, England)\",\"volume\":\"9 1\",\"pages\":\"14\"},\"PeriodicalIF\":4.7000,\"publicationDate\":\"2024-04-06\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10998376/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Advances in simulation (London, England)\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1186/s41077-024-00285-4\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"HEALTH CARE SCIENCES & SERVICES\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Advances in simulation (London, England)","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1186/s41077-024-00285-4","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"HEALTH CARE SCIENCES & SERVICES","Score":null,"Total":0}
Emergency airway management in the prone position: an observational mannequin-based simulation study.
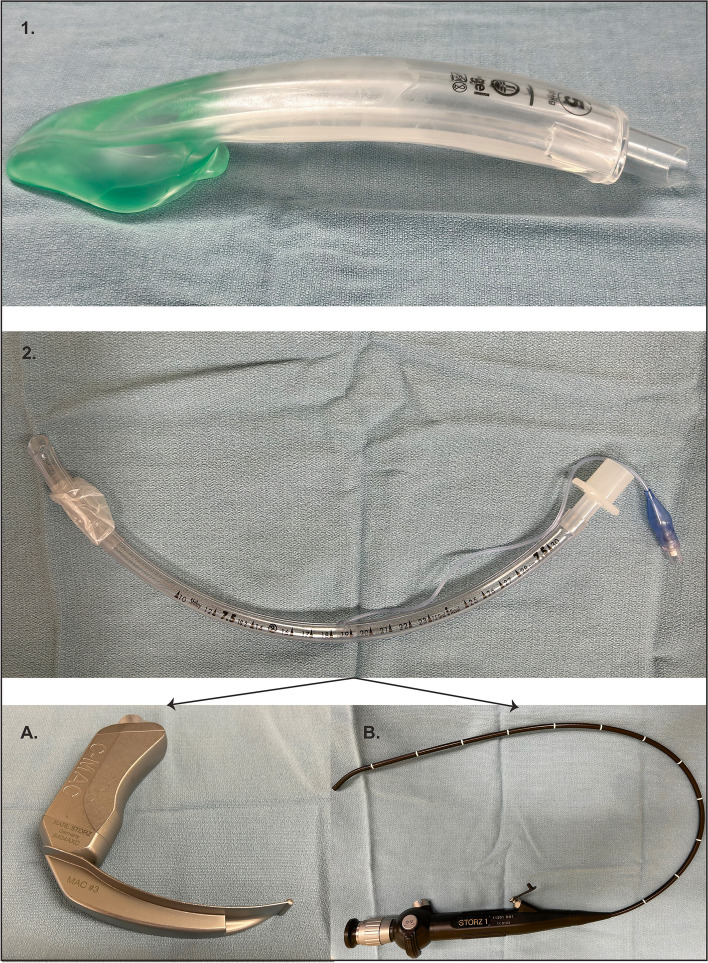
Introduction: Accidental extubation during prone position can be a life-threatening emergency requiring rapid establishment of the airway. However, there is limited evidence of the best airway rescue method for this potentially catastrophic emergency. The aim of this study was to determine the most effective method to recover the airway in case of accidental extubation during prone positioning by comparing three techniques (supraglottic airway, video laryngoscopy, and fiber-optic bronchoscopy) in a simulated environment.
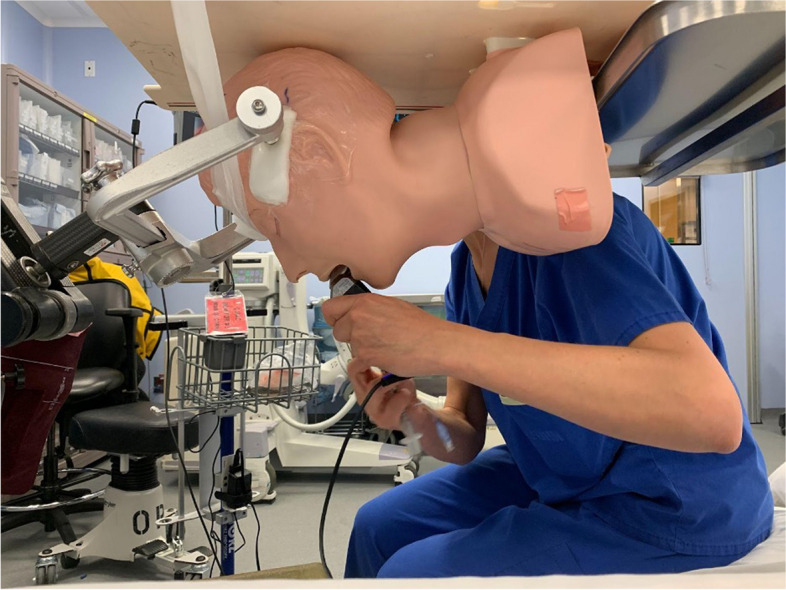
Methods: Eleven anesthesiologists and 12 anesthesia fellows performed the simulated airway management using 3 different techniques on a mannequin positioned prone in head pins. Time required for definitive airway management and the success rates were measured.
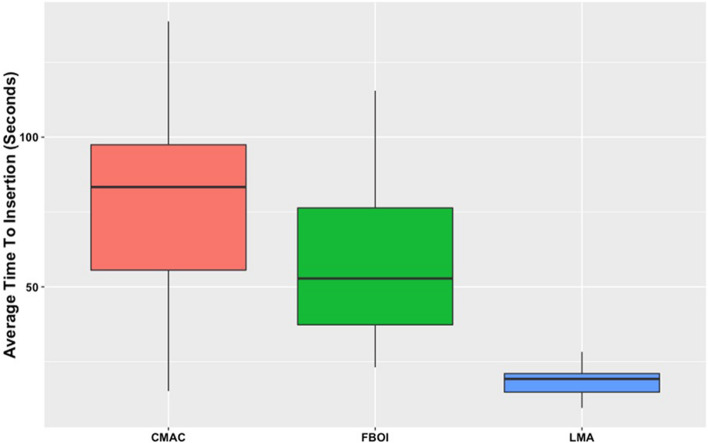
Results: The success rates of airway rescue were 100% with the supraglottic airway device (SAD), 69.6% with the video laryngoscope (CMAC), and 91.3% with the FOB. The mean (SD) time to insertion was 18.1 (4.8) s for the supraglottic airway, 78.3 (32.0) s for the CMAC, and 57.3 (24.6) s for the FOB. There were significant differences in the time required for definitive airway management between the SAD and FOB (t = 5.79, p < 0.001, 95% CI = 25.92-52.38), the SAD and CMAC (t = 8.90, p < 0.001, 95% CI = 46.93-73.40), and the FOB and CMAC (t = 3.11, p = 0.003, 95% CI = 7.78-34.25).
Conclusion: The results of this simulation-based study suggest that the SAD I-gel is the best technique to manage accidental extubation during prone position by establishing a temporary airway with excellent success rate and shorter procedure time. When comparing techniques for securing a definitive airway, the FOB was more successful than the CMAC.



 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
