{"title":"大的非梗阻性结直肠病变片状内镜粘膜切除术后 12 个月首次监测结肠镜检查的安全性。","authors":"","doi":"10.1016/j.gie.2024.05.008","DOIUrl":null,"url":null,"abstract":"<div><h3>Background and Aims</h3><div>After piecemeal EMR (pEMR) of nonpedunculated colorectal lesions ≥20 mm, guidelines recommend first endoscopic surveillance at 6 months. However, initial surveillance at 12 months may be adequate for selected low-risk lesions and could save the cost, risk, and inconvenience of 1 surveillance examination.</div></div><div><h3>Methods</h3><div>This study retrospectively examined a prospectively collected database of all colorectal lesions referred to our center for endoscopic resection between August 2019 and April 2023. We report recurrence rates of patients with colorectal lesions ≥20 mm removed by pEMR who were assigned to 6-month first surveillance or to 12-month first surveillance (or assigned to a 6-month surveillance visit but did not return until after 10 months).</div></div><div><h3>Results</h3><div>There were 561 nonpedunculated lesions ≥20 mm that underwent first follow-up, including 490 lesions in 443 patients assigned to 6-month surveillance and 71 lesions in 65 patients assigned to 12-month surveillance. Lesions assigned to 12-month surveillance were smaller (mean size, 25.9 ± 6.1 mm vs 37.0 ± 17.4 mm), more likely serrated (63.4% vs 9.6%), and more often removed by cold pEMR (74.6% vs 20.4%). Twenty-nine lesions in 24 patients assigned to 6-month surveillance presented after 10 months, and their recurrence data were included in the group assigned to 12-month surveillance. Overall recurrence rates at 6 months and 12 months were 10.0% (46 of 461) and 10.0% (10 of 100), respectively. Mean recurrence sizes at 6 and 12 months were 10.9 ± 6.2 mm and 5.0 ± 3.1 mm, respectively. One patient in the 6-month surveillance group had cancer at the pEMR site, but no other recurrences at 6 or 12 months had either cancer or high-grade dysplasia.</div></div><div><h3>Conclusions</h3><div>Twelve-month surveillance seems acceptable for selected colorectal lesions ≥20 mm removed by pEMR. A randomized trial comparing initial 6-month versus 12-month surveillance is warranted for selected lesions.</div></div>","PeriodicalId":12542,"journal":{"name":"Gastrointestinal endoscopy","volume":"100 5","pages":"Pages 905-913"},"PeriodicalIF":7.5000,"publicationDate":"2024-11-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"","citationCount":"0","resultStr":"{\"title\":\"Safety of first surveillance colonoscopy at 12 months after piecemeal EMR of large nonpedunculated colorectal lesions\",\"authors\":\"\",\"doi\":\"10.1016/j.gie.2024.05.008\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<div><h3>Background and Aims</h3><div>After piecemeal EMR (pEMR) of nonpedunculated colorectal lesions ≥20 mm, guidelines recommend first endoscopic surveillance at 6 months. However, initial surveillance at 12 months may be adequate for selected low-risk lesions and could save the cost, risk, and inconvenience of 1 surveillance examination.</div></div><div><h3>Methods</h3><div>This study retrospectively examined a prospectively collected database of all colorectal lesions referred to our center for endoscopic resection between August 2019 and April 2023. We report recurrence rates of patients with colorectal lesions ≥20 mm removed by pEMR who were assigned to 6-month first surveillance or to 12-month first surveillance (or assigned to a 6-month surveillance visit but did not return until after 10 months).</div></div><div><h3>Results</h3><div>There were 561 nonpedunculated lesions ≥20 mm that underwent first follow-up, including 490 lesions in 443 patients assigned to 6-month surveillance and 71 lesions in 65 patients assigned to 12-month surveillance. Lesions assigned to 12-month surveillance were smaller (mean size, 25.9 ± 6.1 mm vs 37.0 ± 17.4 mm), more likely serrated (63.4% vs 9.6%), and more often removed by cold pEMR (74.6% vs 20.4%). Twenty-nine lesions in 24 patients assigned to 6-month surveillance presented after 10 months, and their recurrence data were included in the group assigned to 12-month surveillance. Overall recurrence rates at 6 months and 12 months were 10.0% (46 of 461) and 10.0% (10 of 100), respectively. Mean recurrence sizes at 6 and 12 months were 10.9 ± 6.2 mm and 5.0 ± 3.1 mm, respectively. One patient in the 6-month surveillance group had cancer at the pEMR site, but no other recurrences at 6 or 12 months had either cancer or high-grade dysplasia.</div></div><div><h3>Conclusions</h3><div>Twelve-month surveillance seems acceptable for selected colorectal lesions ≥20 mm removed by pEMR. A randomized trial comparing initial 6-month versus 12-month surveillance is warranted for selected lesions.</div></div>\",\"PeriodicalId\":12542,\"journal\":{\"name\":\"Gastrointestinal endoscopy\",\"volume\":\"100 5\",\"pages\":\"Pages 905-913\"},\"PeriodicalIF\":7.5000,\"publicationDate\":\"2024-11-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Gastrointestinal endoscopy\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://www.sciencedirect.com/science/article/pii/S0016510724031948\",\"RegionNum\":1,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/5/14 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q1\",\"JCRName\":\"GASTROENTEROLOGY & HEPATOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Gastrointestinal endoscopy","FirstCategoryId":"3","ListUrlMain":"https://www.sciencedirect.com/science/article/pii/S0016510724031948","RegionNum":1,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/5/14 0:00:00","PubModel":"Epub","JCR":"Q1","JCRName":"GASTROENTEROLOGY & HEPATOLOGY","Score":null,"Total":0}
Safety of first surveillance colonoscopy at 12 months after piecemeal EMR of large nonpedunculated colorectal lesions
Background and Aims
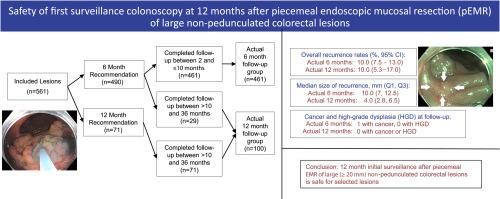
After piecemeal EMR (pEMR) of nonpedunculated colorectal lesions ≥20 mm, guidelines recommend first endoscopic surveillance at 6 months. However, initial surveillance at 12 months may be adequate for selected low-risk lesions and could save the cost, risk, and inconvenience of 1 surveillance examination.
Methods
This study retrospectively examined a prospectively collected database of all colorectal lesions referred to our center for endoscopic resection between August 2019 and April 2023. We report recurrence rates of patients with colorectal lesions ≥20 mm removed by pEMR who were assigned to 6-month first surveillance or to 12-month first surveillance (or assigned to a 6-month surveillance visit but did not return until after 10 months).
Results
There were 561 nonpedunculated lesions ≥20 mm that underwent first follow-up, including 490 lesions in 443 patients assigned to 6-month surveillance and 71 lesions in 65 patients assigned to 12-month surveillance. Lesions assigned to 12-month surveillance were smaller (mean size, 25.9 ± 6.1 mm vs 37.0 ± 17.4 mm), more likely serrated (63.4% vs 9.6%), and more often removed by cold pEMR (74.6% vs 20.4%). Twenty-nine lesions in 24 patients assigned to 6-month surveillance presented after 10 months, and their recurrence data were included in the group assigned to 12-month surveillance. Overall recurrence rates at 6 months and 12 months were 10.0% (46 of 461) and 10.0% (10 of 100), respectively. Mean recurrence sizes at 6 and 12 months were 10.9 ± 6.2 mm and 5.0 ± 3.1 mm, respectively. One patient in the 6-month surveillance group had cancer at the pEMR site, but no other recurrences at 6 or 12 months had either cancer or high-grade dysplasia.
Conclusions
Twelve-month surveillance seems acceptable for selected colorectal lesions ≥20 mm removed by pEMR. A randomized trial comparing initial 6-month versus 12-month surveillance is warranted for selected lesions.
期刊介绍:
Gastrointestinal Endoscopy is a journal publishing original, peer-reviewed articles on endoscopic procedures for studying, diagnosing, and treating digestive diseases. It covers outcomes research, prospective studies, and controlled trials of new endoscopic instruments and treatment methods. The online features include full-text articles, video and audio clips, and MEDLINE links. The journal serves as an international forum for the latest developments in the specialty, offering challenging reports from authorities worldwide. It also publishes abstracts of significant articles from other clinical publications, accompanied by expert commentaries.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
