Jarkko Karvonen, Sanni Lehto, Corinna Lenz, Caroline Beaudoint, Sola Oyeniran, Torsten Kayser, Saila Vikman, Sami Pakarinen
{"title":"分钟通气传感器驱动的心率反应是老年患者心脏再同步疗法优化的一部分。","authors":"Jarkko Karvonen, Sanni Lehto, Corinna Lenz, Caroline Beaudoint, Sola Oyeniran, Torsten Kayser, Saila Vikman, Sami Pakarinen","doi":"10.1007/s10840-024-01848-1","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Chronotropic incompetence (CI) is common among elderly cardiac resynchronization therapy pacemaker (CRT-P) patients on optimal medical therapy. This study aimed to evaluate the impact of optimized rate-adaptive pacing utilizing the minute ventilation (MV) sensor on exercise tolerance.</p><p><strong>Methods: </strong>In a prospective, multicenter study, older patients (median age 76 years) with a guideline-based indication for CRT were evaluated following CRT-P implantation. If there was no documented CI, requiring clinically rate-responsive pacing, the device was programmed DDD at pre-discharge. At 1 month, a 6-min walk test (6MWT) was conducted. If the maximum heart rate was < 100 bpm or < 80% of the age-predicted maximum, the response was considered CI. Patients with CI were programmed with DDDR. At 3 months post-implant, the 6MWT was repeated in the correct respective programming mode. In addition, heart rate score (HRSc, defined as the percentage of all sensed and paced atrial events in the single tallest 10 bpm histogram bin) was assessed at 1 and 3 months.</p><p><strong>Results: </strong>CI was identified in 46/61 (75%) of patients without prior indication at enrollment. MV sensor-based DDDR mode increased heart rate in CI patients similarly to non-CI patients with intrinsically driven heart rates during 6MWT. Walking distance increased substantially with DDDR (349 ± 132 m vs. 376 ± 128 m at 1 and 3 months, respectively, p < 0.05). Furthermore, DDDR reduced HRSc by 14% (absolute reduction, p < 0.001) in those with more severe CI, i.e., HRSc ≥ 70%.</p><p><strong>Conclusion: </strong>Exercise tolerance in older CRT-P patients can be further improved by the utilization of an MV sensor.</p>","PeriodicalId":16202,"journal":{"name":"Journal of Interventional Cardiac Electrophysiology","volume":" ","pages":"2017-2027"},"PeriodicalIF":2.7000,"publicationDate":"2024-12-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11711142/pdf/","citationCount":"0","resultStr":"{\"title\":\"Minute ventilation sensor-driven rate response as a part of cardiac resynchronization therapy optimization in older patients.\",\"authors\":\"Jarkko Karvonen, Sanni Lehto, Corinna Lenz, Caroline Beaudoint, Sola Oyeniran, Torsten Kayser, Saila Vikman, Sami Pakarinen\",\"doi\":\"10.1007/s10840-024-01848-1\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Chronotropic incompetence (CI) is common among elderly cardiac resynchronization therapy pacemaker (CRT-P) patients on optimal medical therapy. This study aimed to evaluate the impact of optimized rate-adaptive pacing utilizing the minute ventilation (MV) sensor on exercise tolerance.</p><p><strong>Methods: </strong>In a prospective, multicenter study, older patients (median age 76 years) with a guideline-based indication for CRT were evaluated following CRT-P implantation. If there was no documented CI, requiring clinically rate-responsive pacing, the device was programmed DDD at pre-discharge. At 1 month, a 6-min walk test (6MWT) was conducted. If the maximum heart rate was < 100 bpm or < 80% of the age-predicted maximum, the response was considered CI. Patients with CI were programmed with DDDR. At 3 months post-implant, the 6MWT was repeated in the correct respective programming mode. In addition, heart rate score (HRSc, defined as the percentage of all sensed and paced atrial events in the single tallest 10 bpm histogram bin) was assessed at 1 and 3 months.</p><p><strong>Results: </strong>CI was identified in 46/61 (75%) of patients without prior indication at enrollment. MV sensor-based DDDR mode increased heart rate in CI patients similarly to non-CI patients with intrinsically driven heart rates during 6MWT. Walking distance increased substantially with DDDR (349 ± 132 m vs. 376 ± 128 m at 1 and 3 months, respectively, p < 0.05). Furthermore, DDDR reduced HRSc by 14% (absolute reduction, p < 0.001) in those with more severe CI, i.e., HRSc ≥ 70%.</p><p><strong>Conclusion: </strong>Exercise tolerance in older CRT-P patients can be further improved by the utilization of an MV sensor.</p>\",\"PeriodicalId\":16202,\"journal\":{\"name\":\"Journal of Interventional Cardiac Electrophysiology\",\"volume\":\" \",\"pages\":\"2017-2027\"},\"PeriodicalIF\":2.7000,\"publicationDate\":\"2024-12-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11711142/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of Interventional Cardiac Electrophysiology\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1007/s10840-024-01848-1\",\"RegionNum\":4,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/6/24 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q3\",\"JCRName\":\"CARDIAC & CARDIOVASCULAR SYSTEMS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Interventional Cardiac Electrophysiology","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1007/s10840-024-01848-1","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/6/24 0:00:00","PubModel":"Epub","JCR":"Q3","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
Minute ventilation sensor-driven rate response as a part of cardiac resynchronization therapy optimization in older patients.
Background: Chronotropic incompetence (CI) is common among elderly cardiac resynchronization therapy pacemaker (CRT-P) patients on optimal medical therapy. This study aimed to evaluate the impact of optimized rate-adaptive pacing utilizing the minute ventilation (MV) sensor on exercise tolerance.
Methods: In a prospective, multicenter study, older patients (median age 76 years) with a guideline-based indication for CRT were evaluated following CRT-P implantation. If there was no documented CI, requiring clinically rate-responsive pacing, the device was programmed DDD at pre-discharge. At 1 month, a 6-min walk test (6MWT) was conducted. If the maximum heart rate was < 100 bpm or < 80% of the age-predicted maximum, the response was considered CI. Patients with CI were programmed with DDDR. At 3 months post-implant, the 6MWT was repeated in the correct respective programming mode. In addition, heart rate score (HRSc, defined as the percentage of all sensed and paced atrial events in the single tallest 10 bpm histogram bin) was assessed at 1 and 3 months.
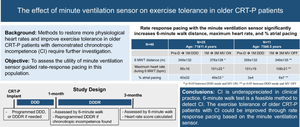
Results: CI was identified in 46/61 (75%) of patients without prior indication at enrollment. MV sensor-based DDDR mode increased heart rate in CI patients similarly to non-CI patients with intrinsically driven heart rates during 6MWT. Walking distance increased substantially with DDDR (349 ± 132 m vs. 376 ± 128 m at 1 and 3 months, respectively, p < 0.05). Furthermore, DDDR reduced HRSc by 14% (absolute reduction, p < 0.001) in those with more severe CI, i.e., HRSc ≥ 70%.
Conclusion: Exercise tolerance in older CRT-P patients can be further improved by the utilization of an MV sensor.
期刊介绍:
The Journal of Interventional Cardiac Electrophysiology is an international publication devoted to fostering research in and development of interventional techniques and therapies for the management of cardiac arrhythmias. It is designed primarily to present original research studies and scholarly scientific reviews of basic and applied science and clinical research in this field. The Journal will adopt a multidisciplinary approach to link physical, experimental, and clinical sciences as applied to the development of and practice in interventional electrophysiology. The Journal will examine techniques ranging from molecular, chemical and pharmacologic therapies to device and ablation technology. Accordingly, original research in clinical, epidemiologic and basic science arenas will be considered for publication. Applied engineering or physical science studies pertaining to interventional electrophysiology will be encouraged. The Journal is committed to providing comprehensive and detailed treatment of major interventional therapies and innovative techniques in a structured and clinically relevant manner. It is directed at clinical practitioners and investigators in the rapidly growing field of interventional electrophysiology. The editorial staff and board reflect this bias and include noted international experts in this area with a wealth of expertise in basic and clinical investigation. Peer review of all submissions, conflict of interest guidelines and periodic editorial board review of all Journal policies have been established.



 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
