John Devaney, Caroline Bradbury-Jones, Amy Charles, Helen L. Daniel, Emily Dobie, Ellen Marks, Katherine Osthwaite, Julie Taylor
{"title":"孩子被带走后产妇过早死亡--利用观察数据的简短报告","authors":"John Devaney, Caroline Bradbury-Jones, Amy Charles, Helen L. Daniel, Emily Dobie, Ellen Marks, Katherine Osthwaite, Julie Taylor","doi":"10.1002/car.2892","DOIUrl":null,"url":null,"abstract":"<p>There continues to be a significant and growing number of children in the care of the state in the United Kingdom (McGhee et al., <span>2017</span>). Children come into state care for a variety of reasons and through a number of different legal routes. Alongside concern about the overall number and the quality of care afforded to some of these children, there are also recurring worries about the immediate and longer term outcomes for this group of children (Duncan, <span>2020</span>; MacAllister, <span>2022</span>). This is not the same as saying that many of these children do not need alternative care.</p><p>There is a common thread of children having experienced a range of adversities, including maltreatment, parental mental ill-health, loss, and poverty, which shape their pre- and in-care experiences, and impact on their social and emotional well-being (Baldwin et al., 2019). While the above issues have been widely researched, there is, however, less information known about the outcomes for children's parents once the child comes into care.</p><p>Over the past decade in the United Kingdom, there has been a growing recognition that some parents, and in particular mothers, experience recurrent removals (Broadhurst & Mason, <span>2013</span>). Research conducted in the United Kingdom and Australia suggests that approximately 20% of women who experience child removal experience repeat court-ordered removals (Broadhurst & Mason, <span>2017</span>; Hinton, <span>2018</span>). In the United Kingdom, this pattern of repeated removals has resulted in the development of services to offer support to address the immediate and successive impacts of such cumulative experiences (Broadhurst et al., <span>2015</span>). Services recognise that birth mothers have been largely offered a reduced level of intervention from children's services (and other sources) once children are removed from their care. This is in spite of the evidence that highlights that childhood adversity resulting in admission to care is often linked to unresolved parental experiences of adversity in their own childhood (Narayan et al., <span>2021</span>), manifesting in trauma symptomatology and behaviours associated with maladaptive coping mechanisms, such as problematic use of prescribed and illicit drugs.</p><p>As such, new approaches to working with mothers seek to offer an intensive rehabilitative response to parents following removal to address the underlying causes of why children needed to be removed, and through addressing the needs of mothers that merges emotional and practical trauma-informed support. As some of these services have been operating for nearly a decade, they have built up both expertise and a significant dataset based on the parents they have worked with. Such services have started to build a picture of the enduring impact on parents of the removal of children into care, as well as existing vulnerabilities prior to removal.</p><p>This paper sets out a collaboration between Pause, a national charity that supports women who have had, or at risk of, recurrent removals of children, and academics from the University of Edinburgh and University of Birmingham, in the United Kingdom. The focus of the paper is the practice-based knowledge that Pause are building regarding the high number of deaths in this community of women with experience of recurrent removals, and what this may, or may not, tell us.</p><p>The Pause programme gives women the chance to pause and take control over their lives, breaking a destructive cycle that causes both them and their children deep trauma. Women are offered up to 18 months of trauma-informed, community-based bespoke support within the context of a relationship within a highly skilled practitioner.</p><p>A review of the research on the health needs of parents in the context of public family care proceedings highlighted that health inequities and poor access to services were apparent across a range of health domains, with longstanding issues often predating legal proceedings or the child's birth (Grant et al., <span>2023</span>). Swedish researchers, using data from a cohort study of individuals born in 1953 and their associated family members, were able to link to administrative data to explore changes in hospitalisation rates due to mental health disorders among parents, 4 years before and after placement of their child in state care. Overall, mothers had higher mean hospitalisation rates than fathers, with both women and men having significantly lower rates of hospitalisation in the 4 years prior to their child's admission to care, compared to the 4 years afterwards (Rajesh et al., <span>2023</span>).</p><p>A Canadian retrospective cohort study using linked administrative data found that mothers who had a child taken into care had significantly higher rates of suicide attempts and completions (Wall-Wieler, Roos, Brownell, et al., <span>2018</span>). The same researchers, using the same data, found that mothers who had a child taken into state care had higher mortality rates compared to their biological sisters who did not have a child taken into care (Wall-Wieler, Roos, Nickel, et al., <span>2018</span>).</p><p>In an editorial for the journal <i>Qualitative Social Work</i>, Morriss and Broadhurst (<span>2022</span>) have called for far greater attention to, and tailoring of provision for, mothers involved with the family courts in the United Kingdom, who are experiencing mental health difficulties. However, the issue seems much broader than this—it is about attending to a range of physical and social emotional needs both during and after legal proceedings, given the evidence to suggest that this may be an indicator of increased risk to death.</p><p>To help local areas decide whether they should set up a Pause Practice in their area (or a similar service supporting parents following the removal of their child), Pause works with local authorities to undertake a scoping exercise that maps the prevalence and pattern of repeated removals of children from women's care in the local area. This exercise is necessary as at present there is no standardised reporting function for local authorities to capture this information; thus, most local authorities cannot tell how many women (and/or men) have had how many children removed from their care. The scoping exercise helps local authorities understand their local level of need and the associated costs that could be avoided by delivering a Pause Practice or another specialist service. Through doing these scoping exercises, Pause started to notice a concerning number of women's deaths, and although this was not the intended purpose of the scoping exercise, were passionate that the findings should not be ignored.</p><p>The data for this paper (Figure 1) is drawn, in part, from 47 scoping exercises, focusing on the ‘Stage 1 Needs assessments’ undertaken by Pause where they have information about women's deaths (the other data are from women Pause has been working with and follows in the ‘Data on women working with Pause’ section). Each needs assessment involves collecting 3–5 years' worth of children's social care data in order to identify the women who have experienced repeated removals of children from their care.</p><p>Pause also reviews case files to provide a summary of presenting issues, although it should be noted that while this provides qualitative information about the complexity of issues faced by the women, it is limited by what can be found about the mothers in the children's files. It does not provide a full picture of the presenting issues and is likely to be a considerable underreport.</p><p>To strengthen the data, Pause also undertakes three deep dive case studies to map the journeys of women who have experienced repeat removals.</p><p>Once data collection has been completed, the data are pseudonymised in order that the analysis undertaken by Pause is anonymous and individual women cannot be identified.</p><p>The purpose of a Pause scoping exercise is to support a local authority to understand their level of need in relation to women who have experienced repeat removals. The information Pause has uncovered about premature deaths of women was not the focus of the scoping exercise, which is why there are gaps in the data. That said, once seen and once understood, the data cannot and should not be ignored.</p><p>In addition to the data from scoping exercises, Pause records when women working with them die. Since 2017, Pause has been notified of 39 women who have died; this is both women Pause was actively working with, and women who had completed the programme but stayed in touch (Table 2).</p><p>To understand more about what they were learning, Pause mapped the women to geographical location in England. They found a fairly even distribution between women from the north of England (<i>n</i> = 21) and women from the south (<i>n</i> = 18), suggesting that the risk of premature death linked to child removal exists across the country. Pause accepts that this is a very crude way of considering where the women live due to the small sample size; however, this reflects that the women that Pause works with are very vulnerable regardless of where they live.</p><p>As noted in Table 3, 19 women died while Pause were actively working with them as part of the 18-month Pause programme. Pause's governance process requires Pause Practices to complete a notification when women die while working with Pause, thus they are aware of the reasons for their deaths (Table 3). The other 20 women died after they had completed the programme or chose to stop working with Pause, and therefore Pause does not have information on cause of death.</p><p>The last 15 years have seen an increasing recognition of the social determinants of health, and the social and structural factors that impact on mortality (Bundy et al., <span>2023</span>; Lewer et al., <span>2020</span>). This paper presents data extending current understandings of the ways that life events, such as the removal of a child from a mother into state care, intersect with existing disadvantages and poor circumstances, such as poor mental health, problematic substance use, and domestic abuse, alongside poverty and racialisation, to cause further health inequities and, ultimately, premature death. The implications of this are twofold. Firstly, there is a moral duty to ensure that parents who have one or more children removed into state care are seen as needing support and care in their own right—not just as extensions of their child's need to be kept safe or rehabilitated to their parent's care. Second, in a compassionate state, there is a public health duty to reduce preventable deaths. In order to do this, there is a clear need to undertake more rigorous research into this phenomenon to better understand the issue, and the potential points of intervention and methods of interventions. There do appear to be different pathways that could usefully be explored. There is strong research evidence of the adversities that many mothers have experienced in their own childhood and prior to their child's removal into care (Narayan et al., <span>2021</span>).</p><p>For some mothers, their death was the result, it appears, of issues that were directly connected to the reasons for their child's need to be in care (such as long-term problematic substance use), whereas for others, the factors leading to death either began or escalated following a child's removal into care (such as a deterioration in their mental health). While local authority children's services should have a responsibility for supporting these women, the expertise and services required will often lie within adult social care and health services.</p><p>Our data are clear in what they show but, as highlighted above, they have been collected for nonresearch purposes and thus are likely to be an under estimation of the actual number of deaths. The degree to which we have robust information on the causes and circumstances of the deaths means that we must be cautious in drawing a linear conclusion between a child's removal and their parent's subsequent premature death. However, notwithstanding these caveats, the data as presented make clear something that has been visible in plain sight—the need to offer support and care to mothers, who are often extremely vulnerable, resulting in their inability to care for their own children. We would propose that larger studies be undertaken, using social care data linked with health statistics, and potentially court records, to more fully identify all the mothers who lose their children for some period of time, and their health trajectory over time, including the timing and cause of their death.</p><p>Mothers who have a child removed from their care often face a range of vulnerabilities, such as experience of childhood abuse, isolation, poverty, poor mental health, domestic abuse, and substance misuse, which contribute to the reasons for their children being removed. Yet following this removal, and at a time of acute need for them due to the trauma involved, birth mothers frequently disappear from the gaze of services, as children's services are structured to meet the needs of the child. The need for support for the children is irrefutable, but equally there needs to be specialist support for their mothers, which goes beyond children's services and needs to involve a key role by health services. The data presented in this paper begin to highlight the significant risks associated with the health inequities that mothers face following the removal of their child: For too many women, these have resulted ultimately in premature death, at a rate of 14 times higher than women their age in the general population based on standard mortality data.</p><p>Further research is needed to understand the national picture of premature deaths for mothers following the removal of their child into care and what steps can be taken to reduce their increased likelihood of dying prematurely. Care proceedings and removal of children should be an alarm bell to all services that the risk of death has increased and therefore they need to respond and support differently. This could include an obligation on local authorities to undertake an assessment of parent's future support and care needs following the granting of a care order, and the convening of a multiagency discussion to look at what support and services are needed. Providing such support would also likely reduce further pregnancies for some women and lessen the need for other children to be removed into care.</p><p>None.</p><p>No independent ethical review of this study was undertaken as the report uses routinely collected administrative data that were anonymised and aggregated by the authors from Pause before sharing with the academic authors.</p>","PeriodicalId":47371,"journal":{"name":"Child Abuse Review","volume":"33 4","pages":""},"PeriodicalIF":1.2000,"publicationDate":"2024-07-09","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1002/car.2892","citationCount":"0","resultStr":"{\"title\":\"Early maternal death following child removal—A short report using observational data\",\"authors\":\"John Devaney, Caroline Bradbury-Jones, Amy Charles, Helen L. Daniel, Emily Dobie, Ellen Marks, Katherine Osthwaite, Julie Taylor\",\"doi\":\"10.1002/car.2892\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p>There continues to be a significant and growing number of children in the care of the state in the United Kingdom (McGhee et al., <span>2017</span>). Children come into state care for a variety of reasons and through a number of different legal routes. Alongside concern about the overall number and the quality of care afforded to some of these children, there are also recurring worries about the immediate and longer term outcomes for this group of children (Duncan, <span>2020</span>; MacAllister, <span>2022</span>). This is not the same as saying that many of these children do not need alternative care.</p><p>There is a common thread of children having experienced a range of adversities, including maltreatment, parental mental ill-health, loss, and poverty, which shape their pre- and in-care experiences, and impact on their social and emotional well-being (Baldwin et al., 2019). While the above issues have been widely researched, there is, however, less information known about the outcomes for children's parents once the child comes into care.</p><p>Over the past decade in the United Kingdom, there has been a growing recognition that some parents, and in particular mothers, experience recurrent removals (Broadhurst & Mason, <span>2013</span>). Research conducted in the United Kingdom and Australia suggests that approximately 20% of women who experience child removal experience repeat court-ordered removals (Broadhurst & Mason, <span>2017</span>; Hinton, <span>2018</span>). In the United Kingdom, this pattern of repeated removals has resulted in the development of services to offer support to address the immediate and successive impacts of such cumulative experiences (Broadhurst et al., <span>2015</span>). Services recognise that birth mothers have been largely offered a reduced level of intervention from children's services (and other sources) once children are removed from their care. This is in spite of the evidence that highlights that childhood adversity resulting in admission to care is often linked to unresolved parental experiences of adversity in their own childhood (Narayan et al., <span>2021</span>), manifesting in trauma symptomatology and behaviours associated with maladaptive coping mechanisms, such as problematic use of prescribed and illicit drugs.</p><p>As such, new approaches to working with mothers seek to offer an intensive rehabilitative response to parents following removal to address the underlying causes of why children needed to be removed, and through addressing the needs of mothers that merges emotional and practical trauma-informed support. As some of these services have been operating for nearly a decade, they have built up both expertise and a significant dataset based on the parents they have worked with. Such services have started to build a picture of the enduring impact on parents of the removal of children into care, as well as existing vulnerabilities prior to removal.</p><p>This paper sets out a collaboration between Pause, a national charity that supports women who have had, or at risk of, recurrent removals of children, and academics from the University of Edinburgh and University of Birmingham, in the United Kingdom. The focus of the paper is the practice-based knowledge that Pause are building regarding the high number of deaths in this community of women with experience of recurrent removals, and what this may, or may not, tell us.</p><p>The Pause programme gives women the chance to pause and take control over their lives, breaking a destructive cycle that causes both them and their children deep trauma. Women are offered up to 18 months of trauma-informed, community-based bespoke support within the context of a relationship within a highly skilled practitioner.</p><p>A review of the research on the health needs of parents in the context of public family care proceedings highlighted that health inequities and poor access to services were apparent across a range of health domains, with longstanding issues often predating legal proceedings or the child's birth (Grant et al., <span>2023</span>). Swedish researchers, using data from a cohort study of individuals born in 1953 and their associated family members, were able to link to administrative data to explore changes in hospitalisation rates due to mental health disorders among parents, 4 years before and after placement of their child in state care. Overall, mothers had higher mean hospitalisation rates than fathers, with both women and men having significantly lower rates of hospitalisation in the 4 years prior to their child's admission to care, compared to the 4 years afterwards (Rajesh et al., <span>2023</span>).</p><p>A Canadian retrospective cohort study using linked administrative data found that mothers who had a child taken into care had significantly higher rates of suicide attempts and completions (Wall-Wieler, Roos, Brownell, et al., <span>2018</span>). The same researchers, using the same data, found that mothers who had a child taken into state care had higher mortality rates compared to their biological sisters who did not have a child taken into care (Wall-Wieler, Roos, Nickel, et al., <span>2018</span>).</p><p>In an editorial for the journal <i>Qualitative Social Work</i>, Morriss and Broadhurst (<span>2022</span>) have called for far greater attention to, and tailoring of provision for, mothers involved with the family courts in the United Kingdom, who are experiencing mental health difficulties. However, the issue seems much broader than this—it is about attending to a range of physical and social emotional needs both during and after legal proceedings, given the evidence to suggest that this may be an indicator of increased risk to death.</p><p>To help local areas decide whether they should set up a Pause Practice in their area (or a similar service supporting parents following the removal of their child), Pause works with local authorities to undertake a scoping exercise that maps the prevalence and pattern of repeated removals of children from women's care in the local area. This exercise is necessary as at present there is no standardised reporting function for local authorities to capture this information; thus, most local authorities cannot tell how many women (and/or men) have had how many children removed from their care. The scoping exercise helps local authorities understand their local level of need and the associated costs that could be avoided by delivering a Pause Practice or another specialist service. Through doing these scoping exercises, Pause started to notice a concerning number of women's deaths, and although this was not the intended purpose of the scoping exercise, were passionate that the findings should not be ignored.</p><p>The data for this paper (Figure 1) is drawn, in part, from 47 scoping exercises, focusing on the ‘Stage 1 Needs assessments’ undertaken by Pause where they have information about women's deaths (the other data are from women Pause has been working with and follows in the ‘Data on women working with Pause’ section). Each needs assessment involves collecting 3–5 years' worth of children's social care data in order to identify the women who have experienced repeated removals of children from their care.</p><p>Pause also reviews case files to provide a summary of presenting issues, although it should be noted that while this provides qualitative information about the complexity of issues faced by the women, it is limited by what can be found about the mothers in the children's files. It does not provide a full picture of the presenting issues and is likely to be a considerable underreport.</p><p>To strengthen the data, Pause also undertakes three deep dive case studies to map the journeys of women who have experienced repeat removals.</p><p>Once data collection has been completed, the data are pseudonymised in order that the analysis undertaken by Pause is anonymous and individual women cannot be identified.</p><p>The purpose of a Pause scoping exercise is to support a local authority to understand their level of need in relation to women who have experienced repeat removals. The information Pause has uncovered about premature deaths of women was not the focus of the scoping exercise, which is why there are gaps in the data. That said, once seen and once understood, the data cannot and should not be ignored.</p><p>In addition to the data from scoping exercises, Pause records when women working with them die. Since 2017, Pause has been notified of 39 women who have died; this is both women Pause was actively working with, and women who had completed the programme but stayed in touch (Table 2).</p><p>To understand more about what they were learning, Pause mapped the women to geographical location in England. They found a fairly even distribution between women from the north of England (<i>n</i> = 21) and women from the south (<i>n</i> = 18), suggesting that the risk of premature death linked to child removal exists across the country. Pause accepts that this is a very crude way of considering where the women live due to the small sample size; however, this reflects that the women that Pause works with are very vulnerable regardless of where they live.</p><p>As noted in Table 3, 19 women died while Pause were actively working with them as part of the 18-month Pause programme. Pause's governance process requires Pause Practices to complete a notification when women die while working with Pause, thus they are aware of the reasons for their deaths (Table 3). The other 20 women died after they had completed the programme or chose to stop working with Pause, and therefore Pause does not have information on cause of death.</p><p>The last 15 years have seen an increasing recognition of the social determinants of health, and the social and structural factors that impact on mortality (Bundy et al., <span>2023</span>; Lewer et al., <span>2020</span>). This paper presents data extending current understandings of the ways that life events, such as the removal of a child from a mother into state care, intersect with existing disadvantages and poor circumstances, such as poor mental health, problematic substance use, and domestic abuse, alongside poverty and racialisation, to cause further health inequities and, ultimately, premature death. The implications of this are twofold. Firstly, there is a moral duty to ensure that parents who have one or more children removed into state care are seen as needing support and care in their own right—not just as extensions of their child's need to be kept safe or rehabilitated to their parent's care. Second, in a compassionate state, there is a public health duty to reduce preventable deaths. In order to do this, there is a clear need to undertake more rigorous research into this phenomenon to better understand the issue, and the potential points of intervention and methods of interventions. There do appear to be different pathways that could usefully be explored. There is strong research evidence of the adversities that many mothers have experienced in their own childhood and prior to their child's removal into care (Narayan et al., <span>2021</span>).</p><p>For some mothers, their death was the result, it appears, of issues that were directly connected to the reasons for their child's need to be in care (such as long-term problematic substance use), whereas for others, the factors leading to death either began or escalated following a child's removal into care (such as a deterioration in their mental health). While local authority children's services should have a responsibility for supporting these women, the expertise and services required will often lie within adult social care and health services.</p><p>Our data are clear in what they show but, as highlighted above, they have been collected for nonresearch purposes and thus are likely to be an under estimation of the actual number of deaths. The degree to which we have robust information on the causes and circumstances of the deaths means that we must be cautious in drawing a linear conclusion between a child's removal and their parent's subsequent premature death. However, notwithstanding these caveats, the data as presented make clear something that has been visible in plain sight—the need to offer support and care to mothers, who are often extremely vulnerable, resulting in their inability to care for their own children. We would propose that larger studies be undertaken, using social care data linked with health statistics, and potentially court records, to more fully identify all the mothers who lose their children for some period of time, and their health trajectory over time, including the timing and cause of their death.</p><p>Mothers who have a child removed from their care often face a range of vulnerabilities, such as experience of childhood abuse, isolation, poverty, poor mental health, domestic abuse, and substance misuse, which contribute to the reasons for their children being removed. Yet following this removal, and at a time of acute need for them due to the trauma involved, birth mothers frequently disappear from the gaze of services, as children's services are structured to meet the needs of the child. The need for support for the children is irrefutable, but equally there needs to be specialist support for their mothers, which goes beyond children's services and needs to involve a key role by health services. The data presented in this paper begin to highlight the significant risks associated with the health inequities that mothers face following the removal of their child: For too many women, these have resulted ultimately in premature death, at a rate of 14 times higher than women their age in the general population based on standard mortality data.</p><p>Further research is needed to understand the national picture of premature deaths for mothers following the removal of their child into care and what steps can be taken to reduce their increased likelihood of dying prematurely. Care proceedings and removal of children should be an alarm bell to all services that the risk of death has increased and therefore they need to respond and support differently. This could include an obligation on local authorities to undertake an assessment of parent's future support and care needs following the granting of a care order, and the convening of a multiagency discussion to look at what support and services are needed. Providing such support would also likely reduce further pregnancies for some women and lessen the need for other children to be removed into care.</p><p>None.</p><p>No independent ethical review of this study was undertaken as the report uses routinely collected administrative data that were anonymised and aggregated by the authors from Pause before sharing with the academic authors.</p>\",\"PeriodicalId\":47371,\"journal\":{\"name\":\"Child Abuse Review\",\"volume\":\"33 4\",\"pages\":\"\"},\"PeriodicalIF\":1.2000,\"publicationDate\":\"2024-07-09\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://onlinelibrary.wiley.com/doi/epdf/10.1002/car.2892\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Child Abuse Review\",\"FirstCategoryId\":\"90\",\"ListUrlMain\":\"https://onlinelibrary.wiley.com/doi/10.1002/car.2892\",\"RegionNum\":4,\"RegionCategory\":\"社会学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q3\",\"JCRName\":\"FAMILY STUDIES\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Child Abuse Review","FirstCategoryId":"90","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/car.2892","RegionNum":4,"RegionCategory":"社会学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"FAMILY STUDIES","Score":null,"Total":0}
Early maternal death following child removal—A short report using observational data
There continues to be a significant and growing number of children in the care of the state in the United Kingdom (McGhee et al., 2017). Children come into state care for a variety of reasons and through a number of different legal routes. Alongside concern about the overall number and the quality of care afforded to some of these children, there are also recurring worries about the immediate and longer term outcomes for this group of children (Duncan, 2020; MacAllister, 2022). This is not the same as saying that many of these children do not need alternative care.
There is a common thread of children having experienced a range of adversities, including maltreatment, parental mental ill-health, loss, and poverty, which shape their pre- and in-care experiences, and impact on their social and emotional well-being (Baldwin et al., 2019). While the above issues have been widely researched, there is, however, less information known about the outcomes for children's parents once the child comes into care.
Over the past decade in the United Kingdom, there has been a growing recognition that some parents, and in particular mothers, experience recurrent removals (Broadhurst & Mason, 2013). Research conducted in the United Kingdom and Australia suggests that approximately 20% of women who experience child removal experience repeat court-ordered removals (Broadhurst & Mason, 2017; Hinton, 2018). In the United Kingdom, this pattern of repeated removals has resulted in the development of services to offer support to address the immediate and successive impacts of such cumulative experiences (Broadhurst et al., 2015). Services recognise that birth mothers have been largely offered a reduced level of intervention from children's services (and other sources) once children are removed from their care. This is in spite of the evidence that highlights that childhood adversity resulting in admission to care is often linked to unresolved parental experiences of adversity in their own childhood (Narayan et al., 2021), manifesting in trauma symptomatology and behaviours associated with maladaptive coping mechanisms, such as problematic use of prescribed and illicit drugs.
As such, new approaches to working with mothers seek to offer an intensive rehabilitative response to parents following removal to address the underlying causes of why children needed to be removed, and through addressing the needs of mothers that merges emotional and practical trauma-informed support. As some of these services have been operating for nearly a decade, they have built up both expertise and a significant dataset based on the parents they have worked with. Such services have started to build a picture of the enduring impact on parents of the removal of children into care, as well as existing vulnerabilities prior to removal.
This paper sets out a collaboration between Pause, a national charity that supports women who have had, or at risk of, recurrent removals of children, and academics from the University of Edinburgh and University of Birmingham, in the United Kingdom. The focus of the paper is the practice-based knowledge that Pause are building regarding the high number of deaths in this community of women with experience of recurrent removals, and what this may, or may not, tell us.
The Pause programme gives women the chance to pause and take control over their lives, breaking a destructive cycle that causes both them and their children deep trauma. Women are offered up to 18 months of trauma-informed, community-based bespoke support within the context of a relationship within a highly skilled practitioner.
A review of the research on the health needs of parents in the context of public family care proceedings highlighted that health inequities and poor access to services were apparent across a range of health domains, with longstanding issues often predating legal proceedings or the child's birth (Grant et al., 2023). Swedish researchers, using data from a cohort study of individuals born in 1953 and their associated family members, were able to link to administrative data to explore changes in hospitalisation rates due to mental health disorders among parents, 4 years before and after placement of their child in state care. Overall, mothers had higher mean hospitalisation rates than fathers, with both women and men having significantly lower rates of hospitalisation in the 4 years prior to their child's admission to care, compared to the 4 years afterwards (Rajesh et al., 2023).
A Canadian retrospective cohort study using linked administrative data found that mothers who had a child taken into care had significantly higher rates of suicide attempts and completions (Wall-Wieler, Roos, Brownell, et al., 2018). The same researchers, using the same data, found that mothers who had a child taken into state care had higher mortality rates compared to their biological sisters who did not have a child taken into care (Wall-Wieler, Roos, Nickel, et al., 2018).
In an editorial for the journal Qualitative Social Work, Morriss and Broadhurst (2022) have called for far greater attention to, and tailoring of provision for, mothers involved with the family courts in the United Kingdom, who are experiencing mental health difficulties. However, the issue seems much broader than this—it is about attending to a range of physical and social emotional needs both during and after legal proceedings, given the evidence to suggest that this may be an indicator of increased risk to death.
To help local areas decide whether they should set up a Pause Practice in their area (or a similar service supporting parents following the removal of their child), Pause works with local authorities to undertake a scoping exercise that maps the prevalence and pattern of repeated removals of children from women's care in the local area. This exercise is necessary as at present there is no standardised reporting function for local authorities to capture this information; thus, most local authorities cannot tell how many women (and/or men) have had how many children removed from their care. The scoping exercise helps local authorities understand their local level of need and the associated costs that could be avoided by delivering a Pause Practice or another specialist service. Through doing these scoping exercises, Pause started to notice a concerning number of women's deaths, and although this was not the intended purpose of the scoping exercise, were passionate that the findings should not be ignored.
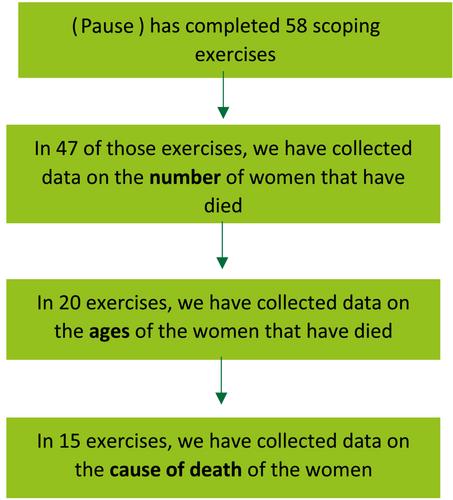
The data for this paper (Figure 1) is drawn, in part, from 47 scoping exercises, focusing on the ‘Stage 1 Needs assessments’ undertaken by Pause where they have information about women's deaths (the other data are from women Pause has been working with and follows in the ‘Data on women working with Pause’ section). Each needs assessment involves collecting 3–5 years' worth of children's social care data in order to identify the women who have experienced repeated removals of children from their care.
Pause also reviews case files to provide a summary of presenting issues, although it should be noted that while this provides qualitative information about the complexity of issues faced by the women, it is limited by what can be found about the mothers in the children's files. It does not provide a full picture of the presenting issues and is likely to be a considerable underreport.
To strengthen the data, Pause also undertakes three deep dive case studies to map the journeys of women who have experienced repeat removals.
Once data collection has been completed, the data are pseudonymised in order that the analysis undertaken by Pause is anonymous and individual women cannot be identified.
The purpose of a Pause scoping exercise is to support a local authority to understand their level of need in relation to women who have experienced repeat removals. The information Pause has uncovered about premature deaths of women was not the focus of the scoping exercise, which is why there are gaps in the data. That said, once seen and once understood, the data cannot and should not be ignored.
In addition to the data from scoping exercises, Pause records when women working with them die. Since 2017, Pause has been notified of 39 women who have died; this is both women Pause was actively working with, and women who had completed the programme but stayed in touch (Table 2).
To understand more about what they were learning, Pause mapped the women to geographical location in England. They found a fairly even distribution between women from the north of England (n = 21) and women from the south (n = 18), suggesting that the risk of premature death linked to child removal exists across the country. Pause accepts that this is a very crude way of considering where the women live due to the small sample size; however, this reflects that the women that Pause works with are very vulnerable regardless of where they live.
As noted in Table 3, 19 women died while Pause were actively working with them as part of the 18-month Pause programme. Pause's governance process requires Pause Practices to complete a notification when women die while working with Pause, thus they are aware of the reasons for their deaths (Table 3). The other 20 women died after they had completed the programme or chose to stop working with Pause, and therefore Pause does not have information on cause of death.
The last 15 years have seen an increasing recognition of the social determinants of health, and the social and structural factors that impact on mortality (Bundy et al., 2023; Lewer et al., 2020). This paper presents data extending current understandings of the ways that life events, such as the removal of a child from a mother into state care, intersect with existing disadvantages and poor circumstances, such as poor mental health, problematic substance use, and domestic abuse, alongside poverty and racialisation, to cause further health inequities and, ultimately, premature death. The implications of this are twofold. Firstly, there is a moral duty to ensure that parents who have one or more children removed into state care are seen as needing support and care in their own right—not just as extensions of their child's need to be kept safe or rehabilitated to their parent's care. Second, in a compassionate state, there is a public health duty to reduce preventable deaths. In order to do this, there is a clear need to undertake more rigorous research into this phenomenon to better understand the issue, and the potential points of intervention and methods of interventions. There do appear to be different pathways that could usefully be explored. There is strong research evidence of the adversities that many mothers have experienced in their own childhood and prior to their child's removal into care (Narayan et al., 2021).
For some mothers, their death was the result, it appears, of issues that were directly connected to the reasons for their child's need to be in care (such as long-term problematic substance use), whereas for others, the factors leading to death either began or escalated following a child's removal into care (such as a deterioration in their mental health). While local authority children's services should have a responsibility for supporting these women, the expertise and services required will often lie within adult social care and health services.
Our data are clear in what they show but, as highlighted above, they have been collected for nonresearch purposes and thus are likely to be an under estimation of the actual number of deaths. The degree to which we have robust information on the causes and circumstances of the deaths means that we must be cautious in drawing a linear conclusion between a child's removal and their parent's subsequent premature death. However, notwithstanding these caveats, the data as presented make clear something that has been visible in plain sight—the need to offer support and care to mothers, who are often extremely vulnerable, resulting in their inability to care for their own children. We would propose that larger studies be undertaken, using social care data linked with health statistics, and potentially court records, to more fully identify all the mothers who lose their children for some period of time, and their health trajectory over time, including the timing and cause of their death.
Mothers who have a child removed from their care often face a range of vulnerabilities, such as experience of childhood abuse, isolation, poverty, poor mental health, domestic abuse, and substance misuse, which contribute to the reasons for their children being removed. Yet following this removal, and at a time of acute need for them due to the trauma involved, birth mothers frequently disappear from the gaze of services, as children's services are structured to meet the needs of the child. The need for support for the children is irrefutable, but equally there needs to be specialist support for their mothers, which goes beyond children's services and needs to involve a key role by health services. The data presented in this paper begin to highlight the significant risks associated with the health inequities that mothers face following the removal of their child: For too many women, these have resulted ultimately in premature death, at a rate of 14 times higher than women their age in the general population based on standard mortality data.
Further research is needed to understand the national picture of premature deaths for mothers following the removal of their child into care and what steps can be taken to reduce their increased likelihood of dying prematurely. Care proceedings and removal of children should be an alarm bell to all services that the risk of death has increased and therefore they need to respond and support differently. This could include an obligation on local authorities to undertake an assessment of parent's future support and care needs following the granting of a care order, and the convening of a multiagency discussion to look at what support and services are needed. Providing such support would also likely reduce further pregnancies for some women and lessen the need for other children to be removed into care.
None.
No independent ethical review of this study was undertaken as the report uses routinely collected administrative data that were anonymised and aggregated by the authors from Pause before sharing with the academic authors.
期刊介绍:
Child Abuse Review provides a forum for all professionals working in the field of child protection, giving them access to the latest research findings, practice developments, training initiatives and policy issues. The Journal"s remit includes all forms of maltreatment, whether they occur inside or outside the family environment. Papers are written in a style appropriate for a multidisciplinary audience and those from outside Britain are welcomed. The Journal maintains a practice orientated focus and authors of research papers are encouraged to examine and discuss implications for practitioners.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
