Matthias Jung, Hanna Rieder, Marco Reisert, Susanne Rospleszcz, Johanna Nattenmueller, Annette Peters, Christopher L. Schlett, Fabian Bamberg, Jakob Weiss
{"title":"骨质疏松症与糖代谢受损之间的关联:深度学习全身磁共振成像群体表型方法","authors":"Matthias Jung, Hanna Rieder, Marco Reisert, Susanne Rospleszcz, Johanna Nattenmueller, Annette Peters, Christopher L. Schlett, Fabian Bamberg, Jakob Weiss","doi":"10.1002/jcsm.13527","DOIUrl":null,"url":null,"abstract":"<div>\n \n \n <section>\n \n <h3> Background</h3>\n \n <p>There is increasing evidence that myosteatosis, which is currently not assessed in clinical routine, plays an important role in risk estimation in individuals with impaired glucose metabolism, as it is associated with the progression of insulin resistance. With advances in artificial intelligence, automated and accurate algorithms have become feasible to fill this gap.</p>\n </section>\n \n <section>\n \n <h3> Methods</h3>\n \n <p>In this retrospective study, we developed and tested a fully automated deep learning model using data from two prospective cohort studies (German National Cohort [NAKO] and Cooperative Health Research in the Region of Augsburg [KORA]) to quantify myosteatosis on whole-body T1-weighted Dixon magnetic resonance imaging as (1) intramuscular adipose tissue (IMAT; the current standard) and (2) quantitative skeletal muscle (SM) fat fraction (SMFF). Subsequently, we investigated the two measures for their discrimination of and association with impaired glucose metabolism beyond baseline demographics (age, sex and body mass index [BMI]) and cardiometabolic risk factors (lipid panel, systolic blood pressure, smoking status and alcohol consumption) in asymptomatic individuals from the KORA study. Impaired glucose metabolism was defined as impaired fasting glucose or impaired glucose tolerance (140–200 mg/dL) or prevalent diabetes mellitus.</p>\n </section>\n \n <section>\n \n <h3> Results</h3>\n \n <p>Model performance was high, with Dice coefficients of ≥0.81 for IMAT and ≥0.91 for SM in the internal (NAKO) and external (KORA) testing sets. In the target population (380 KORA participants: mean age of 53.6 ± 9.2 years, BMI of 28.2 ± 4.9 kg/m<sup>2</sup>, 57.4% male), individuals with impaired glucose metabolism (<i>n</i> = 146; 38.4%) were older and more likely men and showed a higher cardiometabolic risk profile, higher IMAT (4.5 ± 2.2% vs. 3.9 ± 1.7%) and higher SMFF (22.0 ± 4.7% vs. 18.9 ± 3.9%) compared to normoglycaemic controls (all <i>P</i> ≤ 0.005). SMFF showed better discrimination for impaired glucose metabolism than IMAT (area under the receiver operating characteristic curve [AUC] 0.693 vs. 0.582, 95% confidence interval [CI] [0.06–0.16]; <i>P</i> < 0.001) but was not significantly different from BMI (AUC 0.733 vs. 0.693, 95% CI [−0.09 to 0.01]; <i>P</i> = 0.15). In univariable logistic regression, IMAT (odds ratio [OR] = 1.18, 95% CI [1.06–1.32]; <i>P</i> = 0.004) and SMFF (OR = 1.19, 95% CI [1.13–1.26]; <i>P</i> < 0.001) were associated with a higher risk of impaired glucose metabolism. This signal remained robust after multivariable adjustment for baseline demographics and cardiometabolic risk factors for SMFF (OR = 1.10, 95% CI [1.01–1.19]; <i>P</i> = 0.028) but not for IMAT (OR = 1.14, 95% CI [0.97–1.33]; <i>P</i> = 0.11).</p>\n </section>\n \n <section>\n \n <h3> Conclusions</h3>\n \n <p>Quantitative SMFF, but not IMAT, is an independent predictor of impaired glucose metabolism, and discrimination is not significantly different from BMI, making it a promising alternative for the currently established approach. Automated methods such as the proposed model may provide a feasible option for opportunistic screening of myosteatosis and, thus, a low-cost personalized risk assessment solution.</p>\n </section>\n </div>","PeriodicalId":48911,"journal":{"name":"Journal of Cachexia Sarcopenia and Muscle","volume":"15 5","pages":"1750-1760"},"PeriodicalIF":9.9000,"publicationDate":"2024-07-15","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11446675/pdf/","citationCount":"0","resultStr":"{\"title\":\"Association between myosteatosis and impaired glucose metabolism: A deep learning whole-body magnetic resonance imaging population phenotyping approach\",\"authors\":\"Matthias Jung, Hanna Rieder, Marco Reisert, Susanne Rospleszcz, Johanna Nattenmueller, Annette Peters, Christopher L. Schlett, Fabian Bamberg, Jakob Weiss\",\"doi\":\"10.1002/jcsm.13527\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<div>\\n \\n \\n <section>\\n \\n <h3> Background</h3>\\n \\n <p>There is increasing evidence that myosteatosis, which is currently not assessed in clinical routine, plays an important role in risk estimation in individuals with impaired glucose metabolism, as it is associated with the progression of insulin resistance. With advances in artificial intelligence, automated and accurate algorithms have become feasible to fill this gap.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Methods</h3>\\n \\n <p>In this retrospective study, we developed and tested a fully automated deep learning model using data from two prospective cohort studies (German National Cohort [NAKO] and Cooperative Health Research in the Region of Augsburg [KORA]) to quantify myosteatosis on whole-body T1-weighted Dixon magnetic resonance imaging as (1) intramuscular adipose tissue (IMAT; the current standard) and (2) quantitative skeletal muscle (SM) fat fraction (SMFF). Subsequently, we investigated the two measures for their discrimination of and association with impaired glucose metabolism beyond baseline demographics (age, sex and body mass index [BMI]) and cardiometabolic risk factors (lipid panel, systolic blood pressure, smoking status and alcohol consumption) in asymptomatic individuals from the KORA study. Impaired glucose metabolism was defined as impaired fasting glucose or impaired glucose tolerance (140–200 mg/dL) or prevalent diabetes mellitus.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Results</h3>\\n \\n <p>Model performance was high, with Dice coefficients of ≥0.81 for IMAT and ≥0.91 for SM in the internal (NAKO) and external (KORA) testing sets. In the target population (380 KORA participants: mean age of 53.6 ± 9.2 years, BMI of 28.2 ± 4.9 kg/m<sup>2</sup>, 57.4% male), individuals with impaired glucose metabolism (<i>n</i> = 146; 38.4%) were older and more likely men and showed a higher cardiometabolic risk profile, higher IMAT (4.5 ± 2.2% vs. 3.9 ± 1.7%) and higher SMFF (22.0 ± 4.7% vs. 18.9 ± 3.9%) compared to normoglycaemic controls (all <i>P</i> ≤ 0.005). SMFF showed better discrimination for impaired glucose metabolism than IMAT (area under the receiver operating characteristic curve [AUC] 0.693 vs. 0.582, 95% confidence interval [CI] [0.06–0.16]; <i>P</i> < 0.001) but was not significantly different from BMI (AUC 0.733 vs. 0.693, 95% CI [−0.09 to 0.01]; <i>P</i> = 0.15). In univariable logistic regression, IMAT (odds ratio [OR] = 1.18, 95% CI [1.06–1.32]; <i>P</i> = 0.004) and SMFF (OR = 1.19, 95% CI [1.13–1.26]; <i>P</i> < 0.001) were associated with a higher risk of impaired glucose metabolism. This signal remained robust after multivariable adjustment for baseline demographics and cardiometabolic risk factors for SMFF (OR = 1.10, 95% CI [1.01–1.19]; <i>P</i> = 0.028) but not for IMAT (OR = 1.14, 95% CI [0.97–1.33]; <i>P</i> = 0.11).</p>\\n </section>\\n \\n <section>\\n \\n <h3> Conclusions</h3>\\n \\n <p>Quantitative SMFF, but not IMAT, is an independent predictor of impaired glucose metabolism, and discrimination is not significantly different from BMI, making it a promising alternative for the currently established approach. Automated methods such as the proposed model may provide a feasible option for opportunistic screening of myosteatosis and, thus, a low-cost personalized risk assessment solution.</p>\\n </section>\\n </div>\",\"PeriodicalId\":48911,\"journal\":{\"name\":\"Journal of Cachexia Sarcopenia and Muscle\",\"volume\":\"15 5\",\"pages\":\"1750-1760\"},\"PeriodicalIF\":9.9000,\"publicationDate\":\"2024-07-15\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11446675/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of Cachexia Sarcopenia and Muscle\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://onlinelibrary.wiley.com/doi/10.1002/jcsm.13527\",\"RegionNum\":1,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"GERIATRICS & GERONTOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Cachexia Sarcopenia and Muscle","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/jcsm.13527","RegionNum":1,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"GERIATRICS & GERONTOLOGY","Score":null,"Total":0}
引用次数: 0
摘要
背景:越来越多的证据表明,目前在临床常规中尚未评估的骨质疏松症在糖代谢受损患者的风险评估中起着重要作用,因为它与胰岛素抵抗的进展有关。随着人工智能技术的进步,自动化的精确算法已经可以填补这一空白:在这项回顾性研究中,我们利用两项前瞻性队列研究(德国国家队列[NAKO]和奥格斯堡地区合作健康研究[KORA])的数据,开发并测试了一个全自动深度学习模型,将全身 T1 加权迪克森磁共振成像上的肌骨肥大症量化为(1)肌肉内脂肪组织(IMAT;现行标准)和(2)定量骨骼肌(SM)脂肪分数(SMFF)。随后,我们在 KORA 研究的无症状个体中研究了这两种测量方法对葡萄糖代谢受损的辨别力以及与之的关联,而不局限于基线人口统计学指标(年龄、性别和体重指数 [BMI])和心血管代谢风险因素(血脂组合、收缩压、吸烟状况和饮酒量)。糖代谢受损被定义为空腹血糖受损或糖耐量受损(140-200 毫克/分升)或流行性糖尿病:模型性能很高,在内部(NAKO)和外部(KORA)测试集中,IMAT的Dice系数≥0.81,SM的Dice系数≥0.91。在目标人群(380 名 KORA 参与者:平均年龄为 53.6 ± 9.2 岁,体重指数为 28.2 ± 4.9 kg/m2,57.4% 为男性)中,糖代谢受损者(n = 146;38.与正常血糖对照组相比,糖代谢受损者(n = 146;38.4%)年龄更大,更可能是男性,并显示出更高的心脏代谢风险特征、更高的 IMAT(4.5 ± 2.2% vs. 3.9 ± 1.7%)和更高的 SMFF(22.0 ± 4.7% vs. 18.9 ± 3.9%)(所有 P 均≤0.005)。与 IMAT 相比,SMFF 对糖代谢受损的判别能力更强(接收器操作特征曲线下面积 [AUC] 0.693 vs. 0.582,95% 置信区间 [CI] [0.06-0.16];P 结论:SMFF 比 IMAT 更能判别糖代谢受损:定量 SMFF(而非 IMAT)是糖代谢受损的独立预测指标,且与 BMI 的区分度无显著差异,使其有望替代现有方法。自动方法(如所提出的模型)可为肌骨质疏松症的机会性筛查提供一种可行的选择,从而提供一种低成本的个性化风险评估解决方案。
Association between myosteatosis and impaired glucose metabolism: A deep learning whole-body magnetic resonance imaging population phenotyping approach
Background
There is increasing evidence that myosteatosis, which is currently not assessed in clinical routine, plays an important role in risk estimation in individuals with impaired glucose metabolism, as it is associated with the progression of insulin resistance. With advances in artificial intelligence, automated and accurate algorithms have become feasible to fill this gap.
Methods
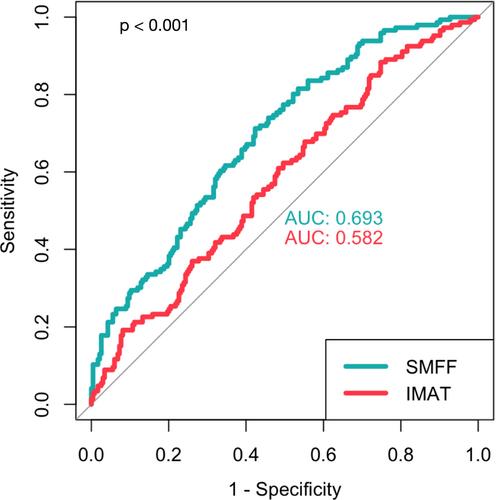
In this retrospective study, we developed and tested a fully automated deep learning model using data from two prospective cohort studies (German National Cohort [NAKO] and Cooperative Health Research in the Region of Augsburg [KORA]) to quantify myosteatosis on whole-body T1-weighted Dixon magnetic resonance imaging as (1) intramuscular adipose tissue (IMAT; the current standard) and (2) quantitative skeletal muscle (SM) fat fraction (SMFF). Subsequently, we investigated the two measures for their discrimination of and association with impaired glucose metabolism beyond baseline demographics (age, sex and body mass index [BMI]) and cardiometabolic risk factors (lipid panel, systolic blood pressure, smoking status and alcohol consumption) in asymptomatic individuals from the KORA study. Impaired glucose metabolism was defined as impaired fasting glucose or impaired glucose tolerance (140–200 mg/dL) or prevalent diabetes mellitus.
Results
Model performance was high, with Dice coefficients of ≥0.81 for IMAT and ≥0.91 for SM in the internal (NAKO) and external (KORA) testing sets. In the target population (380 KORA participants: mean age of 53.6 ± 9.2 years, BMI of 28.2 ± 4.9 kg/m2, 57.4% male), individuals with impaired glucose metabolism (n = 146; 38.4%) were older and more likely men and showed a higher cardiometabolic risk profile, higher IMAT (4.5 ± 2.2% vs. 3.9 ± 1.7%) and higher SMFF (22.0 ± 4.7% vs. 18.9 ± 3.9%) compared to normoglycaemic controls (all P ≤ 0.005). SMFF showed better discrimination for impaired glucose metabolism than IMAT (area under the receiver operating characteristic curve [AUC] 0.693 vs. 0.582, 95% confidence interval [CI] [0.06–0.16]; P < 0.001) but was not significantly different from BMI (AUC 0.733 vs. 0.693, 95% CI [−0.09 to 0.01]; P = 0.15). In univariable logistic regression, IMAT (odds ratio [OR] = 1.18, 95% CI [1.06–1.32]; P = 0.004) and SMFF (OR = 1.19, 95% CI [1.13–1.26]; P < 0.001) were associated with a higher risk of impaired glucose metabolism. This signal remained robust after multivariable adjustment for baseline demographics and cardiometabolic risk factors for SMFF (OR = 1.10, 95% CI [1.01–1.19]; P = 0.028) but not for IMAT (OR = 1.14, 95% CI [0.97–1.33]; P = 0.11).
Conclusions
Quantitative SMFF, but not IMAT, is an independent predictor of impaired glucose metabolism, and discrimination is not significantly different from BMI, making it a promising alternative for the currently established approach. Automated methods such as the proposed model may provide a feasible option for opportunistic screening of myosteatosis and, thus, a low-cost personalized risk assessment solution.
期刊介绍:
The Journal of Cachexia, Sarcopenia and Muscle is a peer-reviewed international journal dedicated to publishing materials related to cachexia and sarcopenia, as well as body composition and its physiological and pathophysiological changes across the lifespan and in response to various illnesses from all fields of life sciences. The journal aims to provide a reliable resource for professionals interested in related research or involved in the clinical care of affected patients, such as those suffering from AIDS, cancer, chronic heart failure, chronic lung disease, liver cirrhosis, chronic kidney failure, rheumatoid arthritis, or sepsis.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
