Marcus Maurer, Hanna Bonnekoh, Eva Grekowitz, Lea Kiefer, Melba Munoz, Manuel P. Pereira, Dorothea Terhorst-Molawi
{"title":"慢性诱发性荨麻疹的诊断和治疗算法,2024 年更新。","authors":"Marcus Maurer, Hanna Bonnekoh, Eva Grekowitz, Lea Kiefer, Melba Munoz, Manuel P. Pereira, Dorothea Terhorst-Molawi","doi":"10.1111/all.16250","DOIUrl":null,"url":null,"abstract":"<p>Chronic inducible urticaria (CIndU) is defined by pruritic wheal formation and/or angioedema in response to a definite and specific trigger.<span><sup>1, 2</sup></span> CIndUs account for 20–30% of all cases of chronic urticaria, that is, urticaria that lasts longer than 6 weeks. Wheals and angioedema, in most types of CIndU, usually occur within 10 min after exposure to the trigger and resolve within 1–3 h after cessation of exposure, except for delayed pressure urticaria (DPU), where symptoms do not appear until hours after exposure to trigger and last up to 24 h. CIndU subtypes are characterized and classified by their specific triggering stimulus, that is, physical and non-physical triggers. Physical stimuli are mechanical friction (symptomatic dermographism), exposure to cold (cold urticaria, ColdU), to heat (heat Urticaria), to components of solar radiation (solar urticaria), pressure (DPU), or vibration (vibratory angioedema). Non-physical stimuli include physical activity (cholinergic urticaria), contact with water (aquagenic urticaria) or to specific agents (contact Urticaria).<span><sup>3</sup></span> In the absence of the specific trigger, symptoms do not develop in CIndU. A discussion of atypical subtypes of CIndU is provided in the supplement.</p><p>The diagnosis of CIndU is built on a thorough patient history and provocation testing (Figure 1). All patients with chronic urticaria, should be asked, “Can you make your wheals come?”, and, if yes, “How?” Depending on the suspected trigger, appropriate provocation testing according to established protocols, with standardized provocation sites, reading times, criteria for positive reactions, and appropriate instruments and documentation, should be performed to confirm the diagnosis (Table 1).<span><sup>4</sup></span> Validated tools for provocation testing are available for most types of CIndU. Antihistamines and glucocorticosteroids should be stopped at least 3 and 7 days before provocation testing, respectively, and testing should not be done at skin sites affected by urticaria in the last 24 h, where the skin may be refractory to whealing.<span><sup>4</sup></span> Provocation testing serves the confirmation of relevant triggers and the assessment of trigger thresholds, which is important for measuring skin susceptibility to trigger-induced whealing as well as monitoring of treatment response. Of note, some CIndU patients, such as those with atypical ColdU, show a negative response to standard provocation testing, despite having a history of trigger-induced whealing.<span><sup>5</sup></span> In these patients, further diagnostic workup is needed.</p><p>CIndU can be challenging to manage and hard to treat, and it often is. In the past, one of the main approaches was to recommend trigger avoidance. However, trigger avoidance is often difficult to achieve for patients.<span><sup>4</sup></span> Current treatment approaches aim to provide complete protection from trigger-induced whealing, until spontaneous remission of the disease occurs (Figure 2). For this approach, the recommended first line therapy is a second generation antihistamine,<span><sup>4</sup></span> which in most cases does not provide complete protection from trigger-induced whealing. Next step is to dose up antihistamines to four times the standard daily dose.<span><sup>3</sup></span> No further licensed drugs are available for CIndU and off-label omalizumab is the recommended second-line treatment option. Further information on the effects of omalizumab and of emerging treatment in CIndU is provided in the supplement, where we also discuss how to manage difficult cases.</p><p>All authors reviewed the literature, drafted, critically reviewed and revised the article, and proofread and approved the final version.</p><p>None.</p><p>Marcus Maurer is or recently was a speaker and/or advisor for and/or has received research funding from Allakos, Alexion, Alvotech, Almirall, Amgen, Aquestive, argenX, AstraZeneca, Celldex, Celltrion, Clinuvel, Escient, Evommune, Excellergy, GSK, Incyte, Jasper, Kashiv, Kyowa Kirin, Leo Pharma, Lilly, Menarini, Mitsubishi Tanabe Pharma, Moxie, Noucor, Novartis, Orion Biotechnology, Resoncance Medicine, Sanofi/Regeneron, Santa Ana Bio, Septerna, Servier, Third HarmonicBio, ValenzaBio, Vitalli Bio, Yuhan Corporation, Zurabio. Hanna Bonnekoh is or recently was, a speaker, advisor and/or received research funding from the following companies: Abbvie, Intercept Pharma, Novartis, Sanofi Aventis, Valenza Bio Inc. Eva Grekowitz was an advisor for Novartis. Lea Kiefer has no conflict of interest. Melba Munoz reports personal fees from Astra Zeneca, Celldex Therapeutics, Takeda, GA2LEN, UNEV, Astra Zeneca and grants from Roche, outside the submitted work. Manuel P. Pereira has received research funding from Almirall; is an investigator for Allakos, Celldex Therapeutics, Incyte, Sanofi and Trevi Therapeutics; and has received consulting fees, speaker honoraria and/or travel fees from AbbVie, Beiersdorf, Celltrion, Doctorflix, Eli Lilly, Falk Foundation, GA2LEN, Galderma, Menlo Therapeutics, Novartis, P.G. Unna Academy, Sanofi, StreamedUP and Trevi Therapeutics. Dorothea Terhorst-Molawi has been an advisor for and/or has received research funding from Moxie, Novartis, Celldex and Sanofi.</p>","PeriodicalId":122,"journal":{"name":"Allergy","volume":"79 9","pages":"2573-2576"},"PeriodicalIF":12.0000,"publicationDate":"2024-07-26","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1111/all.16250","citationCount":"0","resultStr":"{\"title\":\"An algorithm for the diagnosis and treatment of chronic inducible urticaria, 2024 update\",\"authors\":\"Marcus Maurer, Hanna Bonnekoh, Eva Grekowitz, Lea Kiefer, Melba Munoz, Manuel P. Pereira, Dorothea Terhorst-Molawi\",\"doi\":\"10.1111/all.16250\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p>Chronic inducible urticaria (CIndU) is defined by pruritic wheal formation and/or angioedema in response to a definite and specific trigger.<span><sup>1, 2</sup></span> CIndUs account for 20–30% of all cases of chronic urticaria, that is, urticaria that lasts longer than 6 weeks. Wheals and angioedema, in most types of CIndU, usually occur within 10 min after exposure to the trigger and resolve within 1–3 h after cessation of exposure, except for delayed pressure urticaria (DPU), where symptoms do not appear until hours after exposure to trigger and last up to 24 h. CIndU subtypes are characterized and classified by their specific triggering stimulus, that is, physical and non-physical triggers. Physical stimuli are mechanical friction (symptomatic dermographism), exposure to cold (cold urticaria, ColdU), to heat (heat Urticaria), to components of solar radiation (solar urticaria), pressure (DPU), or vibration (vibratory angioedema). Non-physical stimuli include physical activity (cholinergic urticaria), contact with water (aquagenic urticaria) or to specific agents (contact Urticaria).<span><sup>3</sup></span> In the absence of the specific trigger, symptoms do not develop in CIndU. A discussion of atypical subtypes of CIndU is provided in the supplement.</p><p>The diagnosis of CIndU is built on a thorough patient history and provocation testing (Figure 1). All patients with chronic urticaria, should be asked, “Can you make your wheals come?”, and, if yes, “How?” Depending on the suspected trigger, appropriate provocation testing according to established protocols, with standardized provocation sites, reading times, criteria for positive reactions, and appropriate instruments and documentation, should be performed to confirm the diagnosis (Table 1).<span><sup>4</sup></span> Validated tools for provocation testing are available for most types of CIndU. Antihistamines and glucocorticosteroids should be stopped at least 3 and 7 days before provocation testing, respectively, and testing should not be done at skin sites affected by urticaria in the last 24 h, where the skin may be refractory to whealing.<span><sup>4</sup></span> Provocation testing serves the confirmation of relevant triggers and the assessment of trigger thresholds, which is important for measuring skin susceptibility to trigger-induced whealing as well as monitoring of treatment response. Of note, some CIndU patients, such as those with atypical ColdU, show a negative response to standard provocation testing, despite having a history of trigger-induced whealing.<span><sup>5</sup></span> In these patients, further diagnostic workup is needed.</p><p>CIndU can be challenging to manage and hard to treat, and it often is. In the past, one of the main approaches was to recommend trigger avoidance. However, trigger avoidance is often difficult to achieve for patients.<span><sup>4</sup></span> Current treatment approaches aim to provide complete protection from trigger-induced whealing, until spontaneous remission of the disease occurs (Figure 2). For this approach, the recommended first line therapy is a second generation antihistamine,<span><sup>4</sup></span> which in most cases does not provide complete protection from trigger-induced whealing. Next step is to dose up antihistamines to four times the standard daily dose.<span><sup>3</sup></span> No further licensed drugs are available for CIndU and off-label omalizumab is the recommended second-line treatment option. Further information on the effects of omalizumab and of emerging treatment in CIndU is provided in the supplement, where we also discuss how to manage difficult cases.</p><p>All authors reviewed the literature, drafted, critically reviewed and revised the article, and proofread and approved the final version.</p><p>None.</p><p>Marcus Maurer is or recently was a speaker and/or advisor for and/or has received research funding from Allakos, Alexion, Alvotech, Almirall, Amgen, Aquestive, argenX, AstraZeneca, Celldex, Celltrion, Clinuvel, Escient, Evommune, Excellergy, GSK, Incyte, Jasper, Kashiv, Kyowa Kirin, Leo Pharma, Lilly, Menarini, Mitsubishi Tanabe Pharma, Moxie, Noucor, Novartis, Orion Biotechnology, Resoncance Medicine, Sanofi/Regeneron, Santa Ana Bio, Septerna, Servier, Third HarmonicBio, ValenzaBio, Vitalli Bio, Yuhan Corporation, Zurabio. Hanna Bonnekoh is or recently was, a speaker, advisor and/or received research funding from the following companies: Abbvie, Intercept Pharma, Novartis, Sanofi Aventis, Valenza Bio Inc. Eva Grekowitz was an advisor for Novartis. Lea Kiefer has no conflict of interest. Melba Munoz reports personal fees from Astra Zeneca, Celldex Therapeutics, Takeda, GA2LEN, UNEV, Astra Zeneca and grants from Roche, outside the submitted work. Manuel P. Pereira has received research funding from Almirall; is an investigator for Allakos, Celldex Therapeutics, Incyte, Sanofi and Trevi Therapeutics; and has received consulting fees, speaker honoraria and/or travel fees from AbbVie, Beiersdorf, Celltrion, Doctorflix, Eli Lilly, Falk Foundation, GA2LEN, Galderma, Menlo Therapeutics, Novartis, P.G. Unna Academy, Sanofi, StreamedUP and Trevi Therapeutics. Dorothea Terhorst-Molawi has been an advisor for and/or has received research funding from Moxie, Novartis, Celldex and Sanofi.</p>\",\"PeriodicalId\":122,\"journal\":{\"name\":\"Allergy\",\"volume\":\"79 9\",\"pages\":\"2573-2576\"},\"PeriodicalIF\":12.0000,\"publicationDate\":\"2024-07-26\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://onlinelibrary.wiley.com/doi/epdf/10.1111/all.16250\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Allergy\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://onlinelibrary.wiley.com/doi/10.1111/all.16250\",\"RegionNum\":1,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"ALLERGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Allergy","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1111/all.16250","RegionNum":1,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"ALLERGY","Score":null,"Total":0}
An algorithm for the diagnosis and treatment of chronic inducible urticaria, 2024 update
Chronic inducible urticaria (CIndU) is defined by pruritic wheal formation and/or angioedema in response to a definite and specific trigger.1, 2 CIndUs account for 20–30% of all cases of chronic urticaria, that is, urticaria that lasts longer than 6 weeks. Wheals and angioedema, in most types of CIndU, usually occur within 10 min after exposure to the trigger and resolve within 1–3 h after cessation of exposure, except for delayed pressure urticaria (DPU), where symptoms do not appear until hours after exposure to trigger and last up to 24 h. CIndU subtypes are characterized and classified by their specific triggering stimulus, that is, physical and non-physical triggers. Physical stimuli are mechanical friction (symptomatic dermographism), exposure to cold (cold urticaria, ColdU), to heat (heat Urticaria), to components of solar radiation (solar urticaria), pressure (DPU), or vibration (vibratory angioedema). Non-physical stimuli include physical activity (cholinergic urticaria), contact with water (aquagenic urticaria) or to specific agents (contact Urticaria).3 In the absence of the specific trigger, symptoms do not develop in CIndU. A discussion of atypical subtypes of CIndU is provided in the supplement.
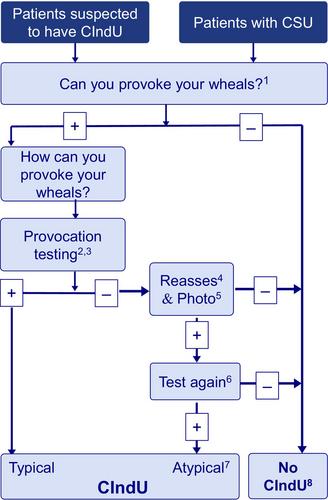
The diagnosis of CIndU is built on a thorough patient history and provocation testing (Figure 1). All patients with chronic urticaria, should be asked, “Can you make your wheals come?”, and, if yes, “How?” Depending on the suspected trigger, appropriate provocation testing according to established protocols, with standardized provocation sites, reading times, criteria for positive reactions, and appropriate instruments and documentation, should be performed to confirm the diagnosis (Table 1).4 Validated tools for provocation testing are available for most types of CIndU. Antihistamines and glucocorticosteroids should be stopped at least 3 and 7 days before provocation testing, respectively, and testing should not be done at skin sites affected by urticaria in the last 24 h, where the skin may be refractory to whealing.4 Provocation testing serves the confirmation of relevant triggers and the assessment of trigger thresholds, which is important for measuring skin susceptibility to trigger-induced whealing as well as monitoring of treatment response. Of note, some CIndU patients, such as those with atypical ColdU, show a negative response to standard provocation testing, despite having a history of trigger-induced whealing.5 In these patients, further diagnostic workup is needed.
CIndU can be challenging to manage and hard to treat, and it often is. In the past, one of the main approaches was to recommend trigger avoidance. However, trigger avoidance is often difficult to achieve for patients.4 Current treatment approaches aim to provide complete protection from trigger-induced whealing, until spontaneous remission of the disease occurs (Figure 2). For this approach, the recommended first line therapy is a second generation antihistamine,4 which in most cases does not provide complete protection from trigger-induced whealing. Next step is to dose up antihistamines to four times the standard daily dose.3 No further licensed drugs are available for CIndU and off-label omalizumab is the recommended second-line treatment option. Further information on the effects of omalizumab and of emerging treatment in CIndU is provided in the supplement, where we also discuss how to manage difficult cases.
All authors reviewed the literature, drafted, critically reviewed and revised the article, and proofread and approved the final version.
None.
Marcus Maurer is or recently was a speaker and/or advisor for and/or has received research funding from Allakos, Alexion, Alvotech, Almirall, Amgen, Aquestive, argenX, AstraZeneca, Celldex, Celltrion, Clinuvel, Escient, Evommune, Excellergy, GSK, Incyte, Jasper, Kashiv, Kyowa Kirin, Leo Pharma, Lilly, Menarini, Mitsubishi Tanabe Pharma, Moxie, Noucor, Novartis, Orion Biotechnology, Resoncance Medicine, Sanofi/Regeneron, Santa Ana Bio, Septerna, Servier, Third HarmonicBio, ValenzaBio, Vitalli Bio, Yuhan Corporation, Zurabio. Hanna Bonnekoh is or recently was, a speaker, advisor and/or received research funding from the following companies: Abbvie, Intercept Pharma, Novartis, Sanofi Aventis, Valenza Bio Inc. Eva Grekowitz was an advisor for Novartis. Lea Kiefer has no conflict of interest. Melba Munoz reports personal fees from Astra Zeneca, Celldex Therapeutics, Takeda, GA2LEN, UNEV, Astra Zeneca and grants from Roche, outside the submitted work. Manuel P. Pereira has received research funding from Almirall; is an investigator for Allakos, Celldex Therapeutics, Incyte, Sanofi and Trevi Therapeutics; and has received consulting fees, speaker honoraria and/or travel fees from AbbVie, Beiersdorf, Celltrion, Doctorflix, Eli Lilly, Falk Foundation, GA2LEN, Galderma, Menlo Therapeutics, Novartis, P.G. Unna Academy, Sanofi, StreamedUP and Trevi Therapeutics. Dorothea Terhorst-Molawi has been an advisor for and/or has received research funding from Moxie, Novartis, Celldex and Sanofi.
期刊介绍:
Allergy is an international and multidisciplinary journal that aims to advance, impact, and communicate all aspects of the discipline of Allergy/Immunology. It publishes original articles, reviews, position papers, guidelines, editorials, news and commentaries, letters to the editors, and correspondences. The journal accepts articles based on their scientific merit and quality.
Allergy seeks to maintain contact between basic and clinical Allergy/Immunology and encourages contributions from contributors and readers from all countries. In addition to its publication, Allergy also provides abstracting and indexing information. Some of the databases that include Allergy abstracts are Abstracts on Hygiene & Communicable Disease, Academic Search Alumni Edition, AgBiotech News & Information, AGRICOLA Database, Biological Abstracts, PubMed Dietary Supplement Subset, and Global Health, among others.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
