{"title":"计算机断层扫描和全身胸透测量肺容量的比较--系统综述。","authors":"Høgni Janus Bjarnason Olsen, Jann Mortensen","doi":"10.1080/20018525.2024.2381898","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Whole-body plethysmography is the preferred method for measuring the static lung volumes: total lung capacity (TLC), functional residual capacity (FRC) and residual volume (RV), as it also incorporates trapped gas - a common finding in chronic obstructive pulmonary disease (COPD). Quantitative computed tomography (CT) is a promising alternative to plethysmography, which can be challenging to perform for patients with severely impaired lung function. The present systematic review explores the agreement between lung volumes measured by plethysmography and CT, as well as the attempts being made to optimize alignment between these two methods.</p><p><strong>Methods: </strong>A literature search was performed on the PubMed database using the block search strategy. Articles were included if they provided both CT based and plethysmography based TLC. Risk of bias was evaluated using the Quality Assessment of Diagnostic Accuracy Studies 2 (QUADAS-2) checklist.</p><p><strong>Results: </strong>22 articles were included. On average, CT-derived TLC (CT-TLC) was 709 mL lower compared to plethysmography TLC (p-TLC) with a 12.1% deviation from the reference standard, p-TLC. This discrepancy (ΔTLC) appeared slightly larger in obstructive patients (obstructive: 781 mL, non-obstructive: 609 mL), whereas percent deviation was slightly smaller (obstructive: 11.4%, non-obstructive: 13.5%). CT-based RV analyses primarily based on COPD patients measured 603 mL higher than plethysmography (p-RV) with 17.8% deviation from p-RV. Studies utilizing spirometry-gating for CT acquisition reported good agreement between modalities (ΔTLC: 70-280 mL), and one study demonstrated noticeable improvements compared to conventional breath-hold instructions in an otherwise identical study setting.</p><p><strong>Conclusion: </strong>CT quantifications routinely underestimate TLC and overestimate RV in comparison to plethysmography. Spirometry gating reduces the level of disagreement and can be of assistance when patients are already undergoing CT. However, further studies are needed to confirm these results.</p>","PeriodicalId":11872,"journal":{"name":"European Clinical Respiratory Journal","volume":"11 1","pages":"2381898"},"PeriodicalIF":1.4000,"publicationDate":"2024-07-29","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11288198/pdf/","citationCount":"0","resultStr":"{\"title\":\"Comparison of lung volumes measured with computed tomography and whole-body plethysmography - a systematic review.\",\"authors\":\"Høgni Janus Bjarnason Olsen, Jann Mortensen\",\"doi\":\"10.1080/20018525.2024.2381898\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Introduction: </strong>Whole-body plethysmography is the preferred method for measuring the static lung volumes: total lung capacity (TLC), functional residual capacity (FRC) and residual volume (RV), as it also incorporates trapped gas - a common finding in chronic obstructive pulmonary disease (COPD). Quantitative computed tomography (CT) is a promising alternative to plethysmography, which can be challenging to perform for patients with severely impaired lung function. The present systematic review explores the agreement between lung volumes measured by plethysmography and CT, as well as the attempts being made to optimize alignment between these two methods.</p><p><strong>Methods: </strong>A literature search was performed on the PubMed database using the block search strategy. Articles were included if they provided both CT based and plethysmography based TLC. Risk of bias was evaluated using the Quality Assessment of Diagnostic Accuracy Studies 2 (QUADAS-2) checklist.</p><p><strong>Results: </strong>22 articles were included. On average, CT-derived TLC (CT-TLC) was 709 mL lower compared to plethysmography TLC (p-TLC) with a 12.1% deviation from the reference standard, p-TLC. This discrepancy (ΔTLC) appeared slightly larger in obstructive patients (obstructive: 781 mL, non-obstructive: 609 mL), whereas percent deviation was slightly smaller (obstructive: 11.4%, non-obstructive: 13.5%). CT-based RV analyses primarily based on COPD patients measured 603 mL higher than plethysmography (p-RV) with 17.8% deviation from p-RV. Studies utilizing spirometry-gating for CT acquisition reported good agreement between modalities (ΔTLC: 70-280 mL), and one study demonstrated noticeable improvements compared to conventional breath-hold instructions in an otherwise identical study setting.</p><p><strong>Conclusion: </strong>CT quantifications routinely underestimate TLC and overestimate RV in comparison to plethysmography. Spirometry gating reduces the level of disagreement and can be of assistance when patients are already undergoing CT. However, further studies are needed to confirm these results.</p>\",\"PeriodicalId\":11872,\"journal\":{\"name\":\"European Clinical Respiratory Journal\",\"volume\":\"11 1\",\"pages\":\"2381898\"},\"PeriodicalIF\":1.4000,\"publicationDate\":\"2024-07-29\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11288198/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"European Clinical Respiratory Journal\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1080/20018525.2024.2381898\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q3\",\"JCRName\":\"RESPIRATORY SYSTEM\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"European Clinical Respiratory Journal","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1080/20018525.2024.2381898","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"RESPIRATORY SYSTEM","Score":null,"Total":0}
Comparison of lung volumes measured with computed tomography and whole-body plethysmography - a systematic review.
Introduction: Whole-body plethysmography is the preferred method for measuring the static lung volumes: total lung capacity (TLC), functional residual capacity (FRC) and residual volume (RV), as it also incorporates trapped gas - a common finding in chronic obstructive pulmonary disease (COPD). Quantitative computed tomography (CT) is a promising alternative to plethysmography, which can be challenging to perform for patients with severely impaired lung function. The present systematic review explores the agreement between lung volumes measured by plethysmography and CT, as well as the attempts being made to optimize alignment between these two methods.
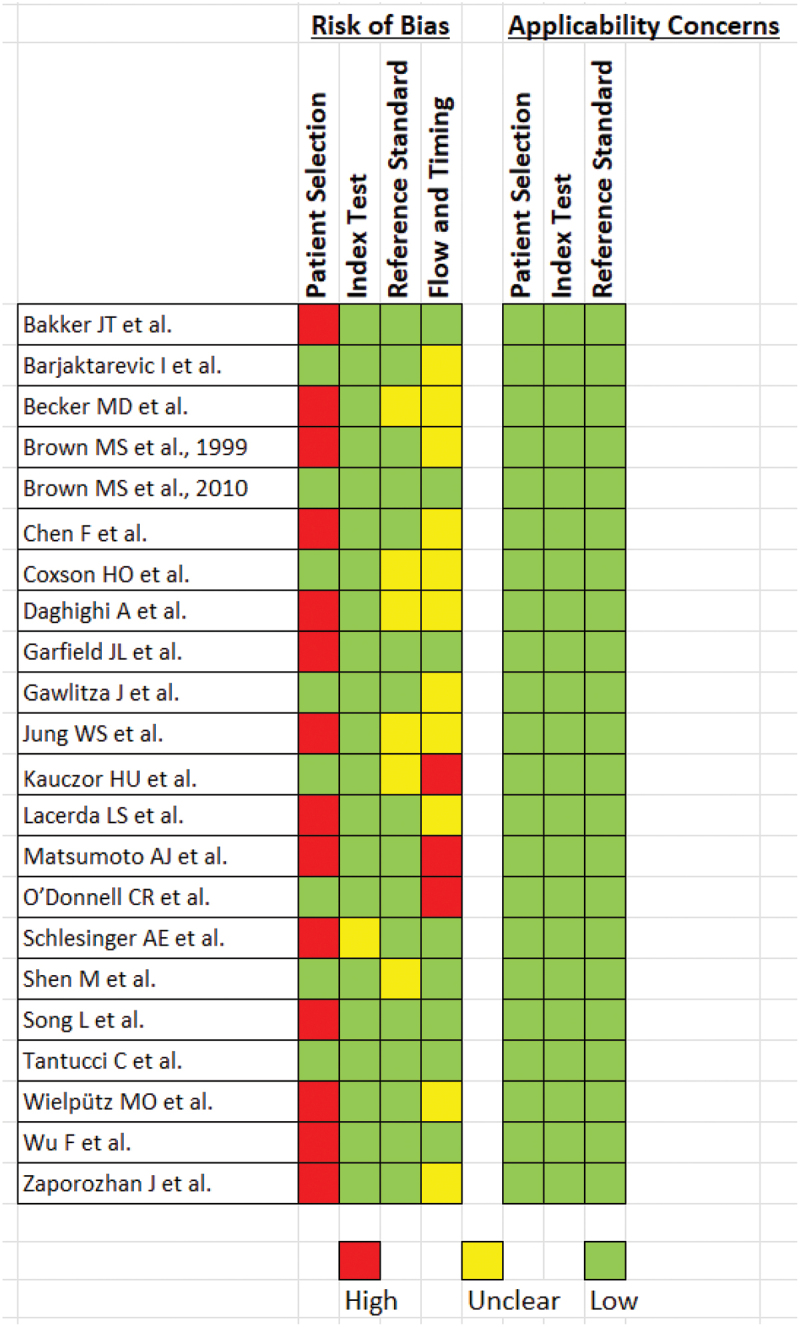
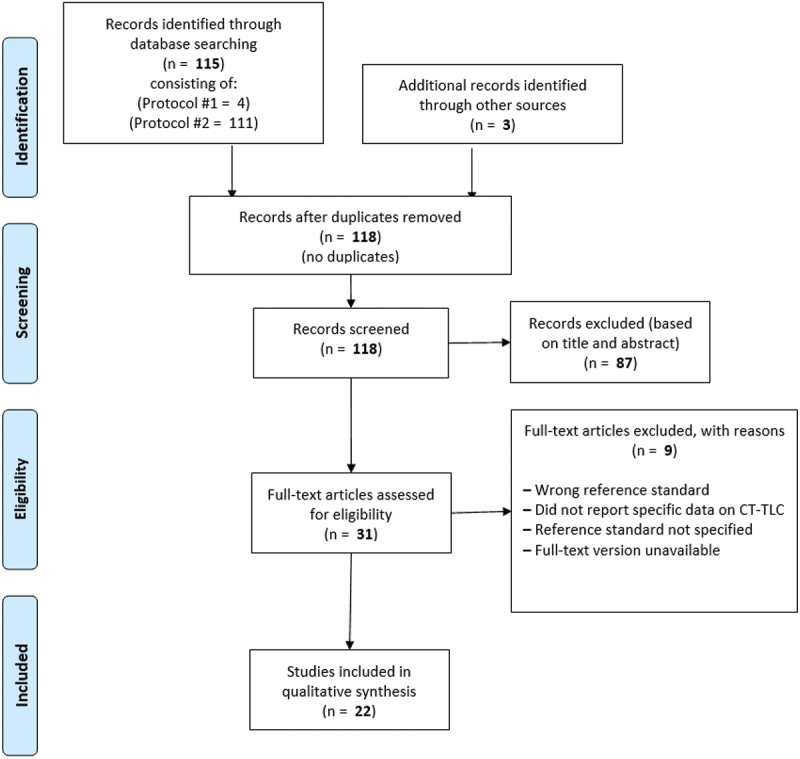
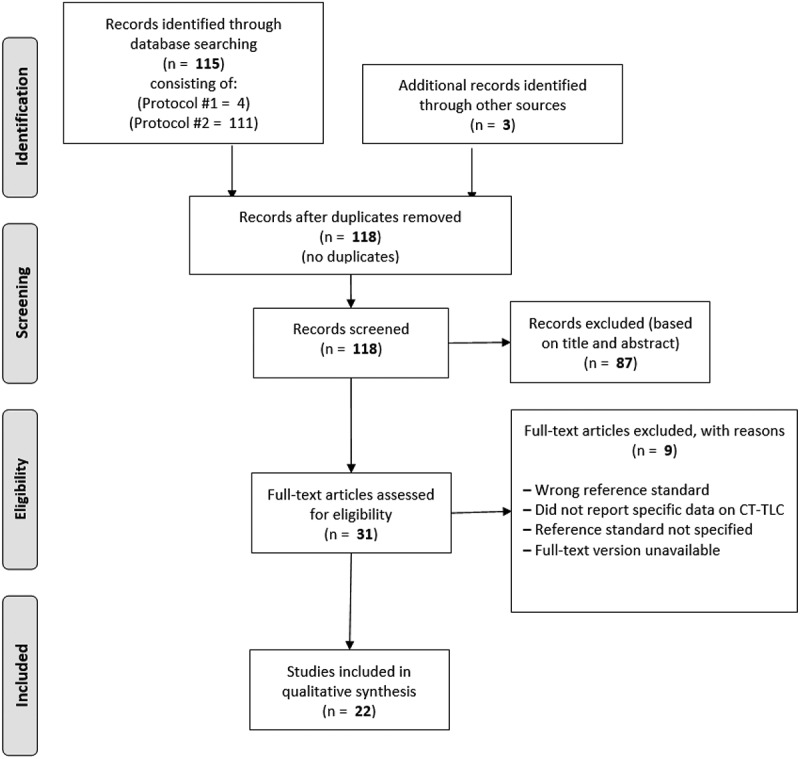
Methods: A literature search was performed on the PubMed database using the block search strategy. Articles were included if they provided both CT based and plethysmography based TLC. Risk of bias was evaluated using the Quality Assessment of Diagnostic Accuracy Studies 2 (QUADAS-2) checklist.
Results: 22 articles were included. On average, CT-derived TLC (CT-TLC) was 709 mL lower compared to plethysmography TLC (p-TLC) with a 12.1% deviation from the reference standard, p-TLC. This discrepancy (ΔTLC) appeared slightly larger in obstructive patients (obstructive: 781 mL, non-obstructive: 609 mL), whereas percent deviation was slightly smaller (obstructive: 11.4%, non-obstructive: 13.5%). CT-based RV analyses primarily based on COPD patients measured 603 mL higher than plethysmography (p-RV) with 17.8% deviation from p-RV. Studies utilizing spirometry-gating for CT acquisition reported good agreement between modalities (ΔTLC: 70-280 mL), and one study demonstrated noticeable improvements compared to conventional breath-hold instructions in an otherwise identical study setting.
Conclusion: CT quantifications routinely underestimate TLC and overestimate RV in comparison to plethysmography. Spirometry gating reduces the level of disagreement and can be of assistance when patients are already undergoing CT. However, further studies are needed to confirm these results.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
