Rachel W Chan, Wilfred W Lam, Hanbo Chen, Leedan Murray, Beibei Zhang, Aimee Theriault, Ruby Endre, Sangkyu Moon, Patrick Liebig, Pejman J Maralani, Chia-Lin Tseng, Sten Myrehaug, Jay Detsky, Mary Jane Lim-Fat, Katrina Roberto, Daniel Djayakarsana, Bharathy Lingamoorthy, Hatef Mehrabian, Benazir Mir Khan, Arjun Sahgal, Hany Soliman, Greg J Stanisz
{"title":"脉冲饱和转移是否足以区分脑转移瘤中的辐射坏死和肿瘤进展?","authors":"Rachel W Chan, Wilfred W Lam, Hanbo Chen, Leedan Murray, Beibei Zhang, Aimee Theriault, Ruby Endre, Sangkyu Moon, Patrick Liebig, Pejman J Maralani, Chia-Lin Tseng, Sten Myrehaug, Jay Detsky, Mary Jane Lim-Fat, Katrina Roberto, Daniel Djayakarsana, Bharathy Lingamoorthy, Hatef Mehrabian, Benazir Mir Khan, Arjun Sahgal, Hany Soliman, Greg J Stanisz","doi":"10.1093/noajnl/vdae132","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Stereotactic radiosurgery (SRS) for the treatment of brain metastases delivers a high dose of radiation with excellent local control but comes with the risk of radiation necrosis (RN), which can be difficult to distinguish from tumor progression (TP). Magnetization transfer (MT) and chemical exchange saturation transfer (CEST) are promising techniques for distinguishing RN from TP in brain metastases. Previous studies used a 2D continuous-wave (ie, block radiofrequency [RF] saturation) MT/CEST approach. The purpose of this study is to investigate a 3D pulsed saturation MT/CEST approach with perfusion MRI for distinguishing RN from TP in brain metastases.</p><p><strong>Methods: </strong>The study included 73 patients scanned with MT/CEST MRI previously treated with SRS or fractionated SRS who developed enhancing lesions with uncertain diagnoses of RN or TP. Perfusion MRI was acquired in 49 of 73 patients. Clinical outcomes were determined by at least 6 months of follow-up or via pathologic confirmation (in 20% of the lesions).</p><p><strong>Results: </strong>Univariable logistic regression resulted in significant variables of the quantitative MT parameter 1/(R<sub>A</sub>·T<sub>2A</sub>), with 5.9 ± 2.7 for RN and 6.5 ± 2.9 for TP. The highest AUC of 75% was obtained using a multivariable logistic regression model for MT/CEST parameters, which included the CEST parameters of AREX<sub>Amide,0.625µT</sub> (<i>P</i> = .013), AREX<sub>NOE,0.625µT</sub> (<i>P</i> = .008), 1/(R<sub>A</sub>·T<sub>2A</sub>) (<i>P</i> = .004), and T<sub>1</sub> (<i>P</i> = .004). The perfusion rCBV parameter did not reach significance.</p><p><strong>Conclusions: </strong>Pulsed saturation transfer was sufficient for achieving a multivariable AUC of 75% for differentiating between RN and TP in brain metastases, but had lower AUCs compared to previous studies that used a block RF approach.</p>","PeriodicalId":94157,"journal":{"name":"Neuro-oncology advances","volume":"6 1","pages":"vdae132"},"PeriodicalIF":4.1000,"publicationDate":"2024-07-29","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11364936/pdf/","citationCount":"0","resultStr":"{\"title\":\"Is pulsed saturation transfer sufficient for differentiating radiation necrosis from tumor progression in brain metastases?\",\"authors\":\"Rachel W Chan, Wilfred W Lam, Hanbo Chen, Leedan Murray, Beibei Zhang, Aimee Theriault, Ruby Endre, Sangkyu Moon, Patrick Liebig, Pejman J Maralani, Chia-Lin Tseng, Sten Myrehaug, Jay Detsky, Mary Jane Lim-Fat, Katrina Roberto, Daniel Djayakarsana, Bharathy Lingamoorthy, Hatef Mehrabian, Benazir Mir Khan, Arjun Sahgal, Hany Soliman, Greg J Stanisz\",\"doi\":\"10.1093/noajnl/vdae132\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Stereotactic radiosurgery (SRS) for the treatment of brain metastases delivers a high dose of radiation with excellent local control but comes with the risk of radiation necrosis (RN), which can be difficult to distinguish from tumor progression (TP). Magnetization transfer (MT) and chemical exchange saturation transfer (CEST) are promising techniques for distinguishing RN from TP in brain metastases. Previous studies used a 2D continuous-wave (ie, block radiofrequency [RF] saturation) MT/CEST approach. The purpose of this study is to investigate a 3D pulsed saturation MT/CEST approach with perfusion MRI for distinguishing RN from TP in brain metastases.</p><p><strong>Methods: </strong>The study included 73 patients scanned with MT/CEST MRI previously treated with SRS or fractionated SRS who developed enhancing lesions with uncertain diagnoses of RN or TP. Perfusion MRI was acquired in 49 of 73 patients. Clinical outcomes were determined by at least 6 months of follow-up or via pathologic confirmation (in 20% of the lesions).</p><p><strong>Results: </strong>Univariable logistic regression resulted in significant variables of the quantitative MT parameter 1/(R<sub>A</sub>·T<sub>2A</sub>), with 5.9 ± 2.7 for RN and 6.5 ± 2.9 for TP. The highest AUC of 75% was obtained using a multivariable logistic regression model for MT/CEST parameters, which included the CEST parameters of AREX<sub>Amide,0.625µT</sub> (<i>P</i> = .013), AREX<sub>NOE,0.625µT</sub> (<i>P</i> = .008), 1/(R<sub>A</sub>·T<sub>2A</sub>) (<i>P</i> = .004), and T<sub>1</sub> (<i>P</i> = .004). The perfusion rCBV parameter did not reach significance.</p><p><strong>Conclusions: </strong>Pulsed saturation transfer was sufficient for achieving a multivariable AUC of 75% for differentiating between RN and TP in brain metastases, but had lower AUCs compared to previous studies that used a block RF approach.</p>\",\"PeriodicalId\":94157,\"journal\":{\"name\":\"Neuro-oncology advances\",\"volume\":\"6 1\",\"pages\":\"vdae132\"},\"PeriodicalIF\":4.1000,\"publicationDate\":\"2024-07-29\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11364936/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Neuro-oncology advances\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1093/noajnl/vdae132\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q1\",\"JCRName\":\"CLINICAL NEUROLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Neuro-oncology advances","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1093/noajnl/vdae132","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/1/1 0:00:00","PubModel":"eCollection","JCR":"Q1","JCRName":"CLINICAL NEUROLOGY","Score":null,"Total":0}
Is pulsed saturation transfer sufficient for differentiating radiation necrosis from tumor progression in brain metastases?
Background: Stereotactic radiosurgery (SRS) for the treatment of brain metastases delivers a high dose of radiation with excellent local control but comes with the risk of radiation necrosis (RN), which can be difficult to distinguish from tumor progression (TP). Magnetization transfer (MT) and chemical exchange saturation transfer (CEST) are promising techniques for distinguishing RN from TP in brain metastases. Previous studies used a 2D continuous-wave (ie, block radiofrequency [RF] saturation) MT/CEST approach. The purpose of this study is to investigate a 3D pulsed saturation MT/CEST approach with perfusion MRI for distinguishing RN from TP in brain metastases.
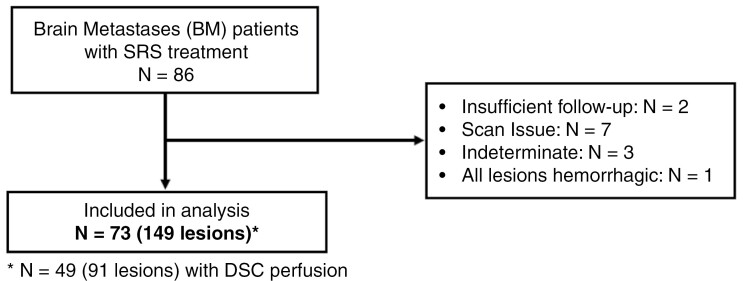
Methods: The study included 73 patients scanned with MT/CEST MRI previously treated with SRS or fractionated SRS who developed enhancing lesions with uncertain diagnoses of RN or TP. Perfusion MRI was acquired in 49 of 73 patients. Clinical outcomes were determined by at least 6 months of follow-up or via pathologic confirmation (in 20% of the lesions).
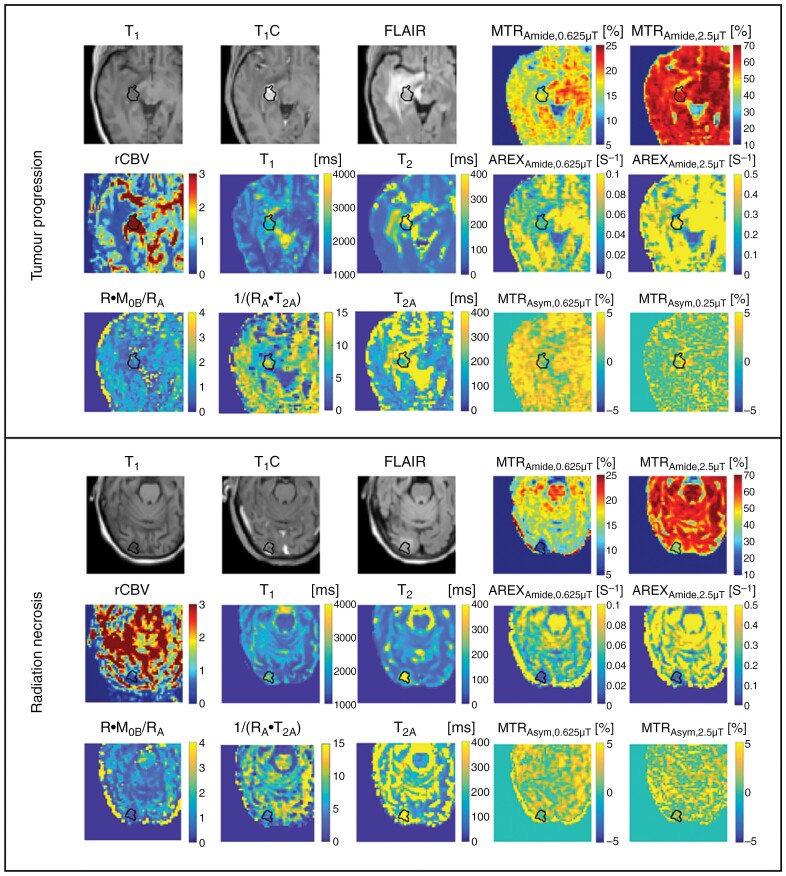
Results: Univariable logistic regression resulted in significant variables of the quantitative MT parameter 1/(RA·T2A), with 5.9 ± 2.7 for RN and 6.5 ± 2.9 for TP. The highest AUC of 75% was obtained using a multivariable logistic regression model for MT/CEST parameters, which included the CEST parameters of AREXAmide,0.625µT (P = .013), AREXNOE,0.625µT (P = .008), 1/(RA·T2A) (P = .004), and T1 (P = .004). The perfusion rCBV parameter did not reach significance.
Conclusions: Pulsed saturation transfer was sufficient for achieving a multivariable AUC of 75% for differentiating between RN and TP in brain metastases, but had lower AUCs compared to previous studies that used a block RF approach.




 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
