Dennis Christoph Harrer , Patricia Mester , Clara-Larissa Lang , Tanja Elger , Tobias Seefeldt , Lorenz Wächter , Judith Dönz , Nina Doblinger , Muriel Huss , Georgios Athanasoulas , Lea U. Krauß , Johannes Heymer , Wolfgang Herr , Tobias Schilling , Stephan Schmid , Martina Müller , Vlad Pavel
{"title":"微创气管造口术(MIT):提高高危重症患者安全性的护理包","authors":"Dennis Christoph Harrer , Patricia Mester , Clara-Larissa Lang , Tanja Elger , Tobias Seefeldt , Lorenz Wächter , Judith Dönz , Nina Doblinger , Muriel Huss , Georgios Athanasoulas , Lea U. Krauß , Johannes Heymer , Wolfgang Herr , Tobias Schilling , Stephan Schmid , Martina Müller , Vlad Pavel","doi":"10.1016/j.jclinane.2024.111631","DOIUrl":null,"url":null,"abstract":"<div><h3>Background</h3><p>Detailed reports are scarce on minimally-invasive tracheostomy (MIT) techniques for critically ill patients with challenging anatomy or complex coagulopathies. In such high-risk patients, conventional percutaneous dilatational tracheostomy (PDT) may lead to severe complications.</p></div><div><h3>Methods</h3><p>Aiming to broaden the scope of MIT for patients previously excluded due to high risks, we developed a new care bundle (MIT technique), specifically designed for intensive care specialists. Our study examined the outcomes of MIT in 32 high-risk patients treated in an ICU of a University Hospital with specific focus on gastrointestinal and liver diseases.</p></div><div><h3>Results</h3><p>We have modified the conventional PDT technique by incorporating an initial skin incision, blunt dissection, diaphanoscopy-guided probe puncture, and continuous bronchoscopic monitoring. Our care bundle also introduces an anterolateral approach for tracheal entry, a significant advancement for patients with complex neck anatomy or dense vasculature, where an anterolateral trajectory avoids midline blood vessels. This enhanced method has proven to be safer than traditional PDT, with a notable absence of post-procedural hemorrhages, cannula misplacements, or infections.</p></div><div><h3>Conclusion</h3><p>The use of our refined care bundle enabled swift minimally-invasive tracheostomy in high-risk patients without the occurrence of serious complications.</p></div>","PeriodicalId":15506,"journal":{"name":"Journal of Clinical Anesthesia","volume":"99 ","pages":"Article 111631"},"PeriodicalIF":5.1000,"publicationDate":"2024-12-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.sciencedirect.com/science/article/pii/S0952818024002605/pdfft?md5=73c90f2ccff19bd45f4af267857f346f&pid=1-s2.0-S0952818024002605-main.pdf","citationCount":"0","resultStr":"{\"title\":\"Minimally-invasive tracheostomy (MIT): A care bundle for safety improvement in high-risk critically ill patients\",\"authors\":\"Dennis Christoph Harrer , Patricia Mester , Clara-Larissa Lang , Tanja Elger , Tobias Seefeldt , Lorenz Wächter , Judith Dönz , Nina Doblinger , Muriel Huss , Georgios Athanasoulas , Lea U. Krauß , Johannes Heymer , Wolfgang Herr , Tobias Schilling , Stephan Schmid , Martina Müller , Vlad Pavel\",\"doi\":\"10.1016/j.jclinane.2024.111631\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<div><h3>Background</h3><p>Detailed reports are scarce on minimally-invasive tracheostomy (MIT) techniques for critically ill patients with challenging anatomy or complex coagulopathies. In such high-risk patients, conventional percutaneous dilatational tracheostomy (PDT) may lead to severe complications.</p></div><div><h3>Methods</h3><p>Aiming to broaden the scope of MIT for patients previously excluded due to high risks, we developed a new care bundle (MIT technique), specifically designed for intensive care specialists. Our study examined the outcomes of MIT in 32 high-risk patients treated in an ICU of a University Hospital with specific focus on gastrointestinal and liver diseases.</p></div><div><h3>Results</h3><p>We have modified the conventional PDT technique by incorporating an initial skin incision, blunt dissection, diaphanoscopy-guided probe puncture, and continuous bronchoscopic monitoring. Our care bundle also introduces an anterolateral approach for tracheal entry, a significant advancement for patients with complex neck anatomy or dense vasculature, where an anterolateral trajectory avoids midline blood vessels. This enhanced method has proven to be safer than traditional PDT, with a notable absence of post-procedural hemorrhages, cannula misplacements, or infections.</p></div><div><h3>Conclusion</h3><p>The use of our refined care bundle enabled swift minimally-invasive tracheostomy in high-risk patients without the occurrence of serious complications.</p></div>\",\"PeriodicalId\":15506,\"journal\":{\"name\":\"Journal of Clinical Anesthesia\",\"volume\":\"99 \",\"pages\":\"Article 111631\"},\"PeriodicalIF\":5.1000,\"publicationDate\":\"2024-12-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.sciencedirect.com/science/article/pii/S0952818024002605/pdfft?md5=73c90f2ccff19bd45f4af267857f346f&pid=1-s2.0-S0952818024002605-main.pdf\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of Clinical Anesthesia\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://www.sciencedirect.com/science/article/pii/S0952818024002605\",\"RegionNum\":2,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/9/21 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q1\",\"JCRName\":\"ANESTHESIOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Clinical Anesthesia","FirstCategoryId":"3","ListUrlMain":"https://www.sciencedirect.com/science/article/pii/S0952818024002605","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/9/21 0:00:00","PubModel":"Epub","JCR":"Q1","JCRName":"ANESTHESIOLOGY","Score":null,"Total":0}
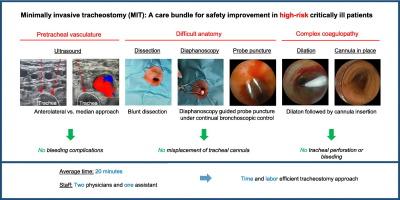
Minimally-invasive tracheostomy (MIT): A care bundle for safety improvement in high-risk critically ill patients
Background
Detailed reports are scarce on minimally-invasive tracheostomy (MIT) techniques for critically ill patients with challenging anatomy or complex coagulopathies. In such high-risk patients, conventional percutaneous dilatational tracheostomy (PDT) may lead to severe complications.
Methods
Aiming to broaden the scope of MIT for patients previously excluded due to high risks, we developed a new care bundle (MIT technique), specifically designed for intensive care specialists. Our study examined the outcomes of MIT in 32 high-risk patients treated in an ICU of a University Hospital with specific focus on gastrointestinal and liver diseases.
Results
We have modified the conventional PDT technique by incorporating an initial skin incision, blunt dissection, diaphanoscopy-guided probe puncture, and continuous bronchoscopic monitoring. Our care bundle also introduces an anterolateral approach for tracheal entry, a significant advancement for patients with complex neck anatomy or dense vasculature, where an anterolateral trajectory avoids midline blood vessels. This enhanced method has proven to be safer than traditional PDT, with a notable absence of post-procedural hemorrhages, cannula misplacements, or infections.
Conclusion
The use of our refined care bundle enabled swift minimally-invasive tracheostomy in high-risk patients without the occurrence of serious complications.
期刊介绍:
The Journal of Clinical Anesthesia (JCA) addresses all aspects of anesthesia practice, including anesthetic administration, pharmacokinetics, preoperative and postoperative considerations, coexisting disease and other complicating factors, cost issues, and similar concerns anesthesiologists contend with daily. Exceptionally high standards of presentation and accuracy are maintained.
The core of the journal is original contributions on subjects relevant to clinical practice, and rigorously peer-reviewed. Highly respected international experts have joined together to form the Editorial Board, sharing their years of experience and clinical expertise. Specialized section editors cover the various subspecialties within the field. To keep your practical clinical skills current, the journal bridges the gap between the laboratory and the clinical practice of anesthesiology and critical care to clarify how new insights can improve daily practice.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
