Francesco Pelliccia, Marco Zimarino, Melania Giordano, Dobromir Dobrev
{"title":"阵发性心房颤动高出血风险患者经皮冠状动脉介入治疗后按需抗凝的可行性:INTERMITTENT 登记。","authors":"Francesco Pelliccia, Marco Zimarino, Melania Giordano, Dobromir Dobrev","doi":"10.1093/ehjdh/ztae046","DOIUrl":null,"url":null,"abstract":"<p><strong>Aims: </strong>This study evaluated the feasibility of the intermittent use of direct oral anticoagulants (DOACs) guided by continuous rhythm monitoring via a clinically validated wearable smart device in high-bleeding risk (HBR) patients with symptomatic paroxysmal atrial fibrillation (AF) otherwise subjected to chronic anticoagulation after percutaneous coronary intervention (PCI).</p><p><strong>Methods and results: </strong>The INTERMITTENT registry was a 3-year prospective observational study at eight Italian centres. Inclusion criteria were elective or urgent PCI, Academic Research Consortium HBR criteria, history of symptomatic 12-lead ECG detected paroxysmal AF episodes, indication to DOACs, and use of a wearable smart device (Apple Watch™). Thirty days after PCI, patients free of AF episodes discontinued DOAC. However, if an AF episode lasting >6 min or a total AF burden > 6 h over 24 h was detected, DOAC was initiated for 30 consecutive days, and withdrawn afterwards if no further AF episodes occurred. At the discretion of the referring physician, intermittent anticoagulation was offered to 89 patients, whereas continuous treatment with DOACs was prescribed to 151 patients. During a follow-up of 298 ± 87 days, the average duration of oral anticoagulation was significantly shorter in the intermittent anticoagulation group (176 ± 43 days, <i>P</i> = 0.0001), representing a 40% reduction in anticoagulation time compared to the continuous group. Ischaemic and bleeding endpoints were not significantly different between the two groups. Propensity score-matching resulted in a total of 69 matched patients with intermittent vs. continuous anticoagulation, respectively. During a follow-up of 291 ± 63 days, there was a significant 46% reduction in anticoagulation time in the intermittent compared to the continuous group (<i>P</i> = 0.0001).</p><p><strong>Conclusion: </strong>In HBR patients with a history of paroxysmal AF episodes who underwent PCI, intermittent anticoagulation guided by continuous rhythm monitoring with a wearable device was feasible and decreased significantly the duration of anticoagulation.</p>","PeriodicalId":72965,"journal":{"name":"European heart journal. Digital health","volume":"5 5","pages":"637-642"},"PeriodicalIF":4.4000,"publicationDate":"2024-06-25","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11417476/pdf/","citationCount":"0","resultStr":"{\"title\":\"Feasibility of anticoagulation on demand after percutaneous coronary intervention in high-bleeding risk patients with paroxysmal atrial fibrillation: the INTERMITTENT registry.\",\"authors\":\"Francesco Pelliccia, Marco Zimarino, Melania Giordano, Dobromir Dobrev\",\"doi\":\"10.1093/ehjdh/ztae046\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Aims: </strong>This study evaluated the feasibility of the intermittent use of direct oral anticoagulants (DOACs) guided by continuous rhythm monitoring via a clinically validated wearable smart device in high-bleeding risk (HBR) patients with symptomatic paroxysmal atrial fibrillation (AF) otherwise subjected to chronic anticoagulation after percutaneous coronary intervention (PCI).</p><p><strong>Methods and results: </strong>The INTERMITTENT registry was a 3-year prospective observational study at eight Italian centres. Inclusion criteria were elective or urgent PCI, Academic Research Consortium HBR criteria, history of symptomatic 12-lead ECG detected paroxysmal AF episodes, indication to DOACs, and use of a wearable smart device (Apple Watch™). Thirty days after PCI, patients free of AF episodes discontinued DOAC. However, if an AF episode lasting >6 min or a total AF burden > 6 h over 24 h was detected, DOAC was initiated for 30 consecutive days, and withdrawn afterwards if no further AF episodes occurred. At the discretion of the referring physician, intermittent anticoagulation was offered to 89 patients, whereas continuous treatment with DOACs was prescribed to 151 patients. During a follow-up of 298 ± 87 days, the average duration of oral anticoagulation was significantly shorter in the intermittent anticoagulation group (176 ± 43 days, <i>P</i> = 0.0001), representing a 40% reduction in anticoagulation time compared to the continuous group. Ischaemic and bleeding endpoints were not significantly different between the two groups. Propensity score-matching resulted in a total of 69 matched patients with intermittent vs. continuous anticoagulation, respectively. During a follow-up of 291 ± 63 days, there was a significant 46% reduction in anticoagulation time in the intermittent compared to the continuous group (<i>P</i> = 0.0001).</p><p><strong>Conclusion: </strong>In HBR patients with a history of paroxysmal AF episodes who underwent PCI, intermittent anticoagulation guided by continuous rhythm monitoring with a wearable device was feasible and decreased significantly the duration of anticoagulation.</p>\",\"PeriodicalId\":72965,\"journal\":{\"name\":\"European heart journal. Digital health\",\"volume\":\"5 5\",\"pages\":\"637-642\"},\"PeriodicalIF\":4.4000,\"publicationDate\":\"2024-06-25\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11417476/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"European heart journal. Digital health\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1093/ehjdh/ztae046\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/9/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q1\",\"JCRName\":\"CARDIAC & CARDIOVASCULAR SYSTEMS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"European heart journal. Digital health","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1093/ehjdh/ztae046","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/9/1 0:00:00","PubModel":"eCollection","JCR":"Q1","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
Feasibility of anticoagulation on demand after percutaneous coronary intervention in high-bleeding risk patients with paroxysmal atrial fibrillation: the INTERMITTENT registry.
Aims: This study evaluated the feasibility of the intermittent use of direct oral anticoagulants (DOACs) guided by continuous rhythm monitoring via a clinically validated wearable smart device in high-bleeding risk (HBR) patients with symptomatic paroxysmal atrial fibrillation (AF) otherwise subjected to chronic anticoagulation after percutaneous coronary intervention (PCI).
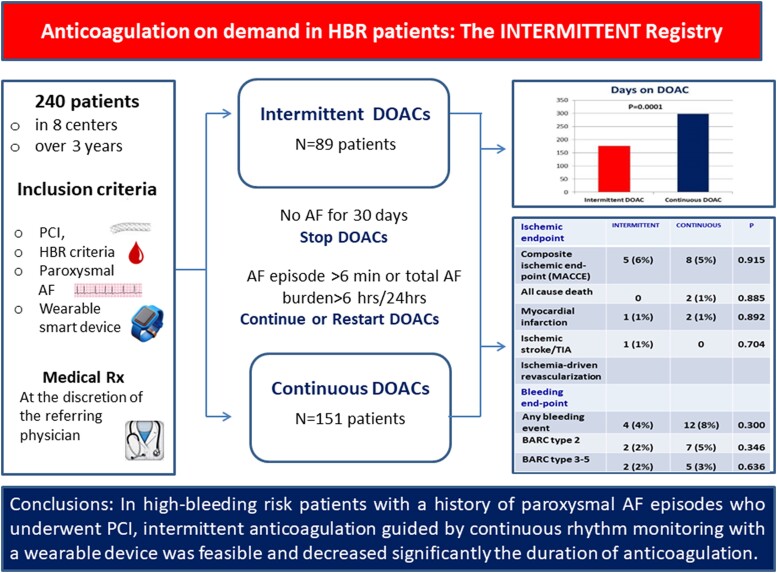
Methods and results: The INTERMITTENT registry was a 3-year prospective observational study at eight Italian centres. Inclusion criteria were elective or urgent PCI, Academic Research Consortium HBR criteria, history of symptomatic 12-lead ECG detected paroxysmal AF episodes, indication to DOACs, and use of a wearable smart device (Apple Watch™). Thirty days after PCI, patients free of AF episodes discontinued DOAC. However, if an AF episode lasting >6 min or a total AF burden > 6 h over 24 h was detected, DOAC was initiated for 30 consecutive days, and withdrawn afterwards if no further AF episodes occurred. At the discretion of the referring physician, intermittent anticoagulation was offered to 89 patients, whereas continuous treatment with DOACs was prescribed to 151 patients. During a follow-up of 298 ± 87 days, the average duration of oral anticoagulation was significantly shorter in the intermittent anticoagulation group (176 ± 43 days, P = 0.0001), representing a 40% reduction in anticoagulation time compared to the continuous group. Ischaemic and bleeding endpoints were not significantly different between the two groups. Propensity score-matching resulted in a total of 69 matched patients with intermittent vs. continuous anticoagulation, respectively. During a follow-up of 291 ± 63 days, there was a significant 46% reduction in anticoagulation time in the intermittent compared to the continuous group (P = 0.0001).
Conclusion: In HBR patients with a history of paroxysmal AF episodes who underwent PCI, intermittent anticoagulation guided by continuous rhythm monitoring with a wearable device was feasible and decreased significantly the duration of anticoagulation.



 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
