Nicolette Sheridan, Karen Hoare, Jenny Carryer, Jane Mills, Sarah Hewitt, Tom Love, Timothy Kenealy
{"title":"护士工作与患者健康结果的关系:比较初级护理模式的观察研究。","authors":"Nicolette Sheridan, Karen Hoare, Jenny Carryer, Jane Mills, Sarah Hewitt, Tom Love, Timothy Kenealy","doi":"10.1186/s12939-024-02288-z","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Māori are over-represented in Aotearoa New Zealand morbidity and mortality statistics. Other populations with high health needs include Pacific peoples and those living with material deprivation. General practice has evolved into seven models of primary care: Traditional, Corporate, Health Care Home, Māori, Pacific, Trusts / Non-governmental organisations (Trust/NGOs) and District Health Board / Primary Care Organisations (DHB/PHO). We describe nurse work in relation to these models of care, populations with high health need and patient health outcomes.</p><p><strong>Methods: </strong>We conducted a cross-sectional study (at 30 September 2018) of data from national datasets and practices at patient level. Six primary outcome measures were selected because they could be improved by primary care: polypharmacy (≥ 65 years), glucose control testing in adults with diabetes, immunisations (at 6 months), ambulatory sensitive hospitalisations (0-14, 45-64 years) and emergency department attendances. Analysis adjusted for patient and practice characteristics.</p><p><strong>Results: </strong>Nurse clinical time, and combined nurse, nurse practitioner and general practitioner clinical time, were substantially higher in Trust/NGO, Māori, and Pacific practices than in other models. Increased patient clinical complexity was associated with more clinical input and higher scores on all outcome measures. The highest rates of preventative care by nurses (cervical screening, cardiovascular risk assessment, depression screening, glucose control testing) were in Māori, Trust/NGO and Pacific practices. There was an eightfold difference, across models of care, in percentage of depression screening undertaken by nurses and a fivefold difference in cervical screening and glucose control testing. The highest rates of nurse consultations afterhours and with unenrolled patients, improving access, were in PHO/DHB, Pacific, Trust/NGO and Māori practices. Work not attributed to nurses in the practice records meant nurse work was underestimated to an unknown degree.</p><p><strong>Conclusions: </strong>Transferring work to nurses in Traditional, Health Care Home, and Corporate practices, would release general practitioner clinical time for other work. Worse patient health outcomes were associated with higher patient need and higher clinical input. It is plausible that there is insufficient clinical input to meet the degree of patient need. More practitioner clinical time is required, especially in practices with high volumes of complex patients.</p>","PeriodicalId":13745,"journal":{"name":"International Journal for Equity in Health","volume":"23 1","pages":"198"},"PeriodicalIF":4.1000,"publicationDate":"2024-10-04","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11451150/pdf/","citationCount":"0","resultStr":"{\"title\":\"Nurses' work in relation to patient health outcomes: an observational study comparing models of primary care.\",\"authors\":\"Nicolette Sheridan, Karen Hoare, Jenny Carryer, Jane Mills, Sarah Hewitt, Tom Love, Timothy Kenealy\",\"doi\":\"10.1186/s12939-024-02288-z\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Māori are over-represented in Aotearoa New Zealand morbidity and mortality statistics. Other populations with high health needs include Pacific peoples and those living with material deprivation. General practice has evolved into seven models of primary care: Traditional, Corporate, Health Care Home, Māori, Pacific, Trusts / Non-governmental organisations (Trust/NGOs) and District Health Board / Primary Care Organisations (DHB/PHO). We describe nurse work in relation to these models of care, populations with high health need and patient health outcomes.</p><p><strong>Methods: </strong>We conducted a cross-sectional study (at 30 September 2018) of data from national datasets and practices at patient level. Six primary outcome measures were selected because they could be improved by primary care: polypharmacy (≥ 65 years), glucose control testing in adults with diabetes, immunisations (at 6 months), ambulatory sensitive hospitalisations (0-14, 45-64 years) and emergency department attendances. Analysis adjusted for patient and practice characteristics.</p><p><strong>Results: </strong>Nurse clinical time, and combined nurse, nurse practitioner and general practitioner clinical time, were substantially higher in Trust/NGO, Māori, and Pacific practices than in other models. Increased patient clinical complexity was associated with more clinical input and higher scores on all outcome measures. The highest rates of preventative care by nurses (cervical screening, cardiovascular risk assessment, depression screening, glucose control testing) were in Māori, Trust/NGO and Pacific practices. There was an eightfold difference, across models of care, in percentage of depression screening undertaken by nurses and a fivefold difference in cervical screening and glucose control testing. The highest rates of nurse consultations afterhours and with unenrolled patients, improving access, were in PHO/DHB, Pacific, Trust/NGO and Māori practices. Work not attributed to nurses in the practice records meant nurse work was underestimated to an unknown degree.</p><p><strong>Conclusions: </strong>Transferring work to nurses in Traditional, Health Care Home, and Corporate practices, would release general practitioner clinical time for other work. Worse patient health outcomes were associated with higher patient need and higher clinical input. It is plausible that there is insufficient clinical input to meet the degree of patient need. More practitioner clinical time is required, especially in practices with high volumes of complex patients.</p>\",\"PeriodicalId\":13745,\"journal\":{\"name\":\"International Journal for Equity in Health\",\"volume\":\"23 1\",\"pages\":\"198\"},\"PeriodicalIF\":4.1000,\"publicationDate\":\"2024-10-04\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11451150/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"International Journal for Equity in Health\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1186/s12939-024-02288-z\",\"RegionNum\":2,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"PUBLIC, ENVIRONMENTAL & OCCUPATIONAL HEALTH\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"International Journal for Equity in Health","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1186/s12939-024-02288-z","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"PUBLIC, ENVIRONMENTAL & OCCUPATIONAL HEALTH","Score":null,"Total":0}
Nurses' work in relation to patient health outcomes: an observational study comparing models of primary care.
Background: Māori are over-represented in Aotearoa New Zealand morbidity and mortality statistics. Other populations with high health needs include Pacific peoples and those living with material deprivation. General practice has evolved into seven models of primary care: Traditional, Corporate, Health Care Home, Māori, Pacific, Trusts / Non-governmental organisations (Trust/NGOs) and District Health Board / Primary Care Organisations (DHB/PHO). We describe nurse work in relation to these models of care, populations with high health need and patient health outcomes.
Methods: We conducted a cross-sectional study (at 30 September 2018) of data from national datasets and practices at patient level. Six primary outcome measures were selected because they could be improved by primary care: polypharmacy (≥ 65 years), glucose control testing in adults with diabetes, immunisations (at 6 months), ambulatory sensitive hospitalisations (0-14, 45-64 years) and emergency department attendances. Analysis adjusted for patient and practice characteristics.
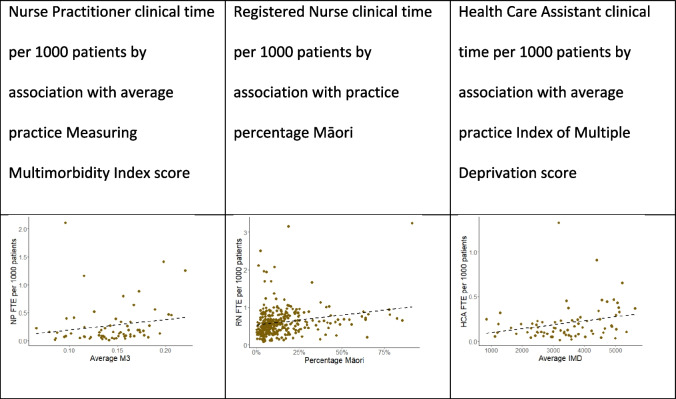
Results: Nurse clinical time, and combined nurse, nurse practitioner and general practitioner clinical time, were substantially higher in Trust/NGO, Māori, and Pacific practices than in other models. Increased patient clinical complexity was associated with more clinical input and higher scores on all outcome measures. The highest rates of preventative care by nurses (cervical screening, cardiovascular risk assessment, depression screening, glucose control testing) were in Māori, Trust/NGO and Pacific practices. There was an eightfold difference, across models of care, in percentage of depression screening undertaken by nurses and a fivefold difference in cervical screening and glucose control testing. The highest rates of nurse consultations afterhours and with unenrolled patients, improving access, were in PHO/DHB, Pacific, Trust/NGO and Māori practices. Work not attributed to nurses in the practice records meant nurse work was underestimated to an unknown degree.
Conclusions: Transferring work to nurses in Traditional, Health Care Home, and Corporate practices, would release general practitioner clinical time for other work. Worse patient health outcomes were associated with higher patient need and higher clinical input. It is plausible that there is insufficient clinical input to meet the degree of patient need. More practitioner clinical time is required, especially in practices with high volumes of complex patients.
期刊介绍:
International Journal for Equity in Health is an Open Access, peer-reviewed, online journal presenting evidence relevant to the search for, and attainment of, equity in health across and within countries. International Journal for Equity in Health aims to improve the understanding of issues that influence the health of populations. This includes the discussion of political, policy-related, economic, social and health services-related influences, particularly with regard to systematic differences in distributions of one or more aspects of health in population groups defined demographically, geographically, or socially.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
