Jack Ettinger, Anita Patel, Julius Ohrnberger, Chris Moore, Manjula Bhudiya, Wayne Smith
{"title":"探索慢性阻塞性肺病患者的偏好,为资源分配提供依据:离散选择实验研究。","authors":"Jack Ettinger, Anita Patel, Julius Ohrnberger, Chris Moore, Manjula Bhudiya, Wayne Smith","doi":"10.1136/bmjresp-2023-001914","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Treatment options for chronic obstructive pulmonary disease (COPD) are numerous but adherence remains a key challenge. We performed a discrete choice experiment (DCE) of patients' preferences in accessing care for the management of COPD. The aim of this study was to understand patients' preferences for modes of accessing care for the management of COPD. This piece of work was then used to inform resource allocation decisions in five integrated care systems (ICSs) in England.</p><p><strong>Methods: </strong>People with diagnosed COPD in five ICSs were invited to complete an online survey from August to September 2022. An experimental design built on the principles of minimal overlap, level balance and orthogonality was used to create 20 sets of 11 scenarios for participants to assess. Participants were presented with three hypothetical options and asked to select their most preferred or state that none was preferred. Data were analysed using a hierarchal Bayes algorithm.</p><p><strong>Results: </strong>Of 82 639 patients with COPD in the study area, 520 completed the survey. The mean health-related quality of life score derived using EuroQol 5-Dimensions 5-Level was 0.57 (0.29). The attributes assigned greatest importance were treatment outcomes, treatment delivery and the type of staff who deliver treatment. Mean utility level scores were substantially higher for little relief (22.75 (SD 78.80)) or some relief from symptoms (20.67 (46.77)) than for complete relief (‒43.42 (83.03)). Of the treatment delivery options, in-person individual appointments were preferred (mean utility score 48.34 (SD 48.14)), and care being provided by healthcare professionals was viewed as very important (77.50 (64.39)).</p><p><strong>Conclusions: </strong>The DCE approach can help resource allocation decisions by indicating attributes most important to patients and trade-offs they are willing to make in treatment access and delivery.</p>","PeriodicalId":9048,"journal":{"name":"BMJ Open Respiratory Research","volume":"11 1","pages":""},"PeriodicalIF":3.4000,"publicationDate":"2024-10-09","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11474863/pdf/","citationCount":"0","resultStr":"{\"title\":\"Exploration of preferences among people with COPD to inform resource allocation: a discrete choice experiment study.\",\"authors\":\"Jack Ettinger, Anita Patel, Julius Ohrnberger, Chris Moore, Manjula Bhudiya, Wayne Smith\",\"doi\":\"10.1136/bmjresp-2023-001914\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Introduction: </strong>Treatment options for chronic obstructive pulmonary disease (COPD) are numerous but adherence remains a key challenge. We performed a discrete choice experiment (DCE) of patients' preferences in accessing care for the management of COPD. The aim of this study was to understand patients' preferences for modes of accessing care for the management of COPD. This piece of work was then used to inform resource allocation decisions in five integrated care systems (ICSs) in England.</p><p><strong>Methods: </strong>People with diagnosed COPD in five ICSs were invited to complete an online survey from August to September 2022. An experimental design built on the principles of minimal overlap, level balance and orthogonality was used to create 20 sets of 11 scenarios for participants to assess. Participants were presented with three hypothetical options and asked to select their most preferred or state that none was preferred. Data were analysed using a hierarchal Bayes algorithm.</p><p><strong>Results: </strong>Of 82 639 patients with COPD in the study area, 520 completed the survey. The mean health-related quality of life score derived using EuroQol 5-Dimensions 5-Level was 0.57 (0.29). The attributes assigned greatest importance were treatment outcomes, treatment delivery and the type of staff who deliver treatment. Mean utility level scores were substantially higher for little relief (22.75 (SD 78.80)) or some relief from symptoms (20.67 (46.77)) than for complete relief (‒43.42 (83.03)). Of the treatment delivery options, in-person individual appointments were preferred (mean utility score 48.34 (SD 48.14)), and care being provided by healthcare professionals was viewed as very important (77.50 (64.39)).</p><p><strong>Conclusions: </strong>The DCE approach can help resource allocation decisions by indicating attributes most important to patients and trade-offs they are willing to make in treatment access and delivery.</p>\",\"PeriodicalId\":9048,\"journal\":{\"name\":\"BMJ Open Respiratory Research\",\"volume\":\"11 1\",\"pages\":\"\"},\"PeriodicalIF\":3.4000,\"publicationDate\":\"2024-10-09\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11474863/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"BMJ Open Respiratory Research\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1136/bmjresp-2023-001914\",\"RegionNum\":3,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"RESPIRATORY SYSTEM\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"BMJ Open Respiratory Research","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1136/bmjresp-2023-001914","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"RESPIRATORY SYSTEM","Score":null,"Total":0}
Exploration of preferences among people with COPD to inform resource allocation: a discrete choice experiment study.
Introduction: Treatment options for chronic obstructive pulmonary disease (COPD) are numerous but adherence remains a key challenge. We performed a discrete choice experiment (DCE) of patients' preferences in accessing care for the management of COPD. The aim of this study was to understand patients' preferences for modes of accessing care for the management of COPD. This piece of work was then used to inform resource allocation decisions in five integrated care systems (ICSs) in England.
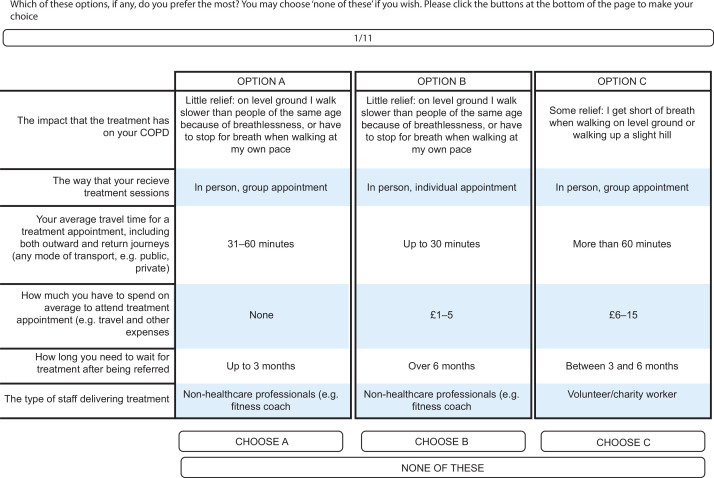
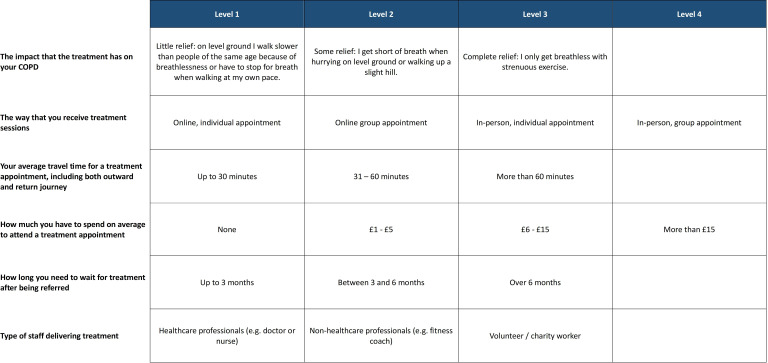
Methods: People with diagnosed COPD in five ICSs were invited to complete an online survey from August to September 2022. An experimental design built on the principles of minimal overlap, level balance and orthogonality was used to create 20 sets of 11 scenarios for participants to assess. Participants were presented with three hypothetical options and asked to select their most preferred or state that none was preferred. Data were analysed using a hierarchal Bayes algorithm.
Results: Of 82 639 patients with COPD in the study area, 520 completed the survey. The mean health-related quality of life score derived using EuroQol 5-Dimensions 5-Level was 0.57 (0.29). The attributes assigned greatest importance were treatment outcomes, treatment delivery and the type of staff who deliver treatment. Mean utility level scores were substantially higher for little relief (22.75 (SD 78.80)) or some relief from symptoms (20.67 (46.77)) than for complete relief (‒43.42 (83.03)). Of the treatment delivery options, in-person individual appointments were preferred (mean utility score 48.34 (SD 48.14)), and care being provided by healthcare professionals was viewed as very important (77.50 (64.39)).
Conclusions: The DCE approach can help resource allocation decisions by indicating attributes most important to patients and trade-offs they are willing to make in treatment access and delivery.
期刊介绍:
BMJ Open Respiratory Research is a peer-reviewed, open access journal publishing respiratory and critical care medicine. It is the sister journal to Thorax and co-owned by the British Thoracic Society and BMJ. The journal focuses on robustness of methodology and scientific rigour with less emphasis on novelty or perceived impact. BMJ Open Respiratory Research operates a rapid review process, with continuous publication online, ensuring timely, up-to-date research is available worldwide. The journal publishes review articles and all research study types: Basic science including laboratory based experiments and animal models, Pilot studies or proof of concept, Observational studies, Study protocols, Registries, Clinical trials from phase I to multicentre randomised clinical trials, Systematic reviews and meta-analyses.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
