Meiqi Shi, Ping Chen, Bin Cui, Yuanhu Yao, Juanyi Wang, Tong Zhou, Li Wang
{"title":"表皮生长因子受体 TKIs 治疗失败后,表皮生长因子受体阳性晚期 NSCLC 患者使用本迈斯托巴特和安罗替尼:I/II 期研究","authors":"Meiqi Shi, Ping Chen, Bin Cui, Yuanhu Yao, Juanyi Wang, Tong Zhou, Li Wang","doi":"10.1038/s41392-024-01982-2","DOIUrl":null,"url":null,"abstract":"<p>The effect of immune‐based therapies on patients with epidermal growth factor receptor (EGFR)-positive advanced non-small cell lung cancer (NSCLC) resistant to EGFR tyrosine kinase inhibitor (TKI) therapy remains unclear. The ALTER-L038 study aimed to evaluate efficacy and safety of a chemotherapy-free combination of benmelstobart, an anti-programmed cell death ligand 1 antibody, and anlotinib, a small-molecule multi-target anti-angiogenic TKI, in EGFR-positive advanced NSCLC patients who progressed after EGFR TKI therapy. Patients were enrolled in a phase I/II study. In phase I (dose-escalation), patients received anlotinib (8, 10, 12 mg) plus benmelstobart (1200 mg). Recommended phase II dose, determined during phase I, was used in phase II dose-expansion cohort. Primary endpoints were maximum tolerable dose in phase I and progression-free survival (PFS) in phase II. At the data cutoff date (March 10, 2024), 55 patients were enrolled in phase II dose-expansion cohort. Median PFS of patients included in phase II cohort was 9.0 months, median overall survival was 28.9 months, objective response rate was 25.5%, disease control rate was 87.3%, and median duration of response was 19.8 months. Incidence of grade ≥3 treatment-related adverse events in study population was 25.5% (14/55), whereas grade ≥3 immune-related adverse events occurred in 10.9% (6/55) of patients. Benmelstobart plus anlotinib showed promising anti-tumor efficacy with tolerable safety profile, supporting the value of further development of this convenient chemotherapy-free regimen for patients with EGFR-positive advanced NSCLC who progressed after EGFR TKI therapy. Trial Registration: ChiCTR1900026273.</p>","PeriodicalId":21766,"journal":{"name":"Signal Transduction and Targeted Therapy","volume":"24 1","pages":""},"PeriodicalIF":52.7000,"publicationDate":"2024-10-10","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"","citationCount":"0","resultStr":"{\"title\":\"Benmelstobart plus anlotinib in patients with EGFR-positive advanced NSCLC after failure of EGFR TKIs therapy: a phase I/II study\",\"authors\":\"Meiqi Shi, Ping Chen, Bin Cui, Yuanhu Yao, Juanyi Wang, Tong Zhou, Li Wang\",\"doi\":\"10.1038/s41392-024-01982-2\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p>The effect of immune‐based therapies on patients with epidermal growth factor receptor (EGFR)-positive advanced non-small cell lung cancer (NSCLC) resistant to EGFR tyrosine kinase inhibitor (TKI) therapy remains unclear. The ALTER-L038 study aimed to evaluate efficacy and safety of a chemotherapy-free combination of benmelstobart, an anti-programmed cell death ligand 1 antibody, and anlotinib, a small-molecule multi-target anti-angiogenic TKI, in EGFR-positive advanced NSCLC patients who progressed after EGFR TKI therapy. Patients were enrolled in a phase I/II study. In phase I (dose-escalation), patients received anlotinib (8, 10, 12 mg) plus benmelstobart (1200 mg). Recommended phase II dose, determined during phase I, was used in phase II dose-expansion cohort. Primary endpoints were maximum tolerable dose in phase I and progression-free survival (PFS) in phase II. At the data cutoff date (March 10, 2024), 55 patients were enrolled in phase II dose-expansion cohort. Median PFS of patients included in phase II cohort was 9.0 months, median overall survival was 28.9 months, objective response rate was 25.5%, disease control rate was 87.3%, and median duration of response was 19.8 months. Incidence of grade ≥3 treatment-related adverse events in study population was 25.5% (14/55), whereas grade ≥3 immune-related adverse events occurred in 10.9% (6/55) of patients. Benmelstobart plus anlotinib showed promising anti-tumor efficacy with tolerable safety profile, supporting the value of further development of this convenient chemotherapy-free regimen for patients with EGFR-positive advanced NSCLC who progressed after EGFR TKI therapy. Trial Registration: ChiCTR1900026273.</p>\",\"PeriodicalId\":21766,\"journal\":{\"name\":\"Signal Transduction and Targeted Therapy\",\"volume\":\"24 1\",\"pages\":\"\"},\"PeriodicalIF\":52.7000,\"publicationDate\":\"2024-10-10\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Signal Transduction and Targeted Therapy\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1038/s41392-024-01982-2\",\"RegionNum\":1,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"BIOCHEMISTRY & MOLECULAR BIOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Signal Transduction and Targeted Therapy","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1038/s41392-024-01982-2","RegionNum":1,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"BIOCHEMISTRY & MOLECULAR BIOLOGY","Score":null,"Total":0}
引用次数: 0
摘要
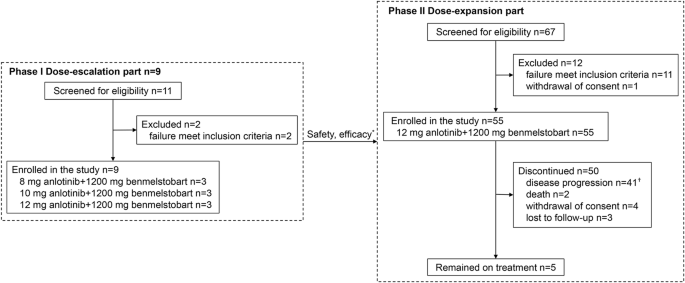
免疫疗法对表皮生长因子受体(EGFR)阳性、对EGFR酪氨酸激酶抑制剂(TKI)疗法耐药的晚期非小细胞肺癌(NSCLC)患者的疗效仍不明确。ALTER-L038研究旨在评估抗程序性细胞死亡配体1抗体benmelstobart和小分子多靶点抗血管生成TKI安罗替尼免化疗联合疗法对经EGFR TKI治疗后病情进展的EGFR阳性晚期NSCLC患者的疗效和安全性。患者被纳入 I/II 期研究。在 I 期(剂量递增期),患者接受安罗替尼(8、10、12 毫克)加苯麦斯多巴(1200 毫克)治疗。II期剂量扩展队列采用I期确定的II期推荐剂量。主要终点是I期的最大耐受剂量和II期的无进展生存期(PFS)。截至数据截止日(2024 年 3 月 10 日),有 55 名患者加入了 II 期剂量扩展队列。II期队列患者的中位无生存期为9.0个月,中位总生存期为28.9个月,客观反应率为25.5%,疾病控制率为87.3%,中位反应持续时间为19.8个月。研究人群中≥3级治疗相关不良事件发生率为25.5%(14/55),而≥3级免疫相关不良事件发生率为10.9%(6/55)。本迈斯托巴特联合安罗替尼显示出良好的抗肿瘤疗效和可耐受的安全性,支持进一步开发这种便捷的无化疗方案,用于EGFR TKI治疗后进展的EGFR阳性晚期NSCLC患者。试验注册:ChiCTR1900026273。
Benmelstobart plus anlotinib in patients with EGFR-positive advanced NSCLC after failure of EGFR TKIs therapy: a phase I/II study
The effect of immune‐based therapies on patients with epidermal growth factor receptor (EGFR)-positive advanced non-small cell lung cancer (NSCLC) resistant to EGFR tyrosine kinase inhibitor (TKI) therapy remains unclear. The ALTER-L038 study aimed to evaluate efficacy and safety of a chemotherapy-free combination of benmelstobart, an anti-programmed cell death ligand 1 antibody, and anlotinib, a small-molecule multi-target anti-angiogenic TKI, in EGFR-positive advanced NSCLC patients who progressed after EGFR TKI therapy. Patients were enrolled in a phase I/II study. In phase I (dose-escalation), patients received anlotinib (8, 10, 12 mg) plus benmelstobart (1200 mg). Recommended phase II dose, determined during phase I, was used in phase II dose-expansion cohort. Primary endpoints were maximum tolerable dose in phase I and progression-free survival (PFS) in phase II. At the data cutoff date (March 10, 2024), 55 patients were enrolled in phase II dose-expansion cohort. Median PFS of patients included in phase II cohort was 9.0 months, median overall survival was 28.9 months, objective response rate was 25.5%, disease control rate was 87.3%, and median duration of response was 19.8 months. Incidence of grade ≥3 treatment-related adverse events in study population was 25.5% (14/55), whereas grade ≥3 immune-related adverse events occurred in 10.9% (6/55) of patients. Benmelstobart plus anlotinib showed promising anti-tumor efficacy with tolerable safety profile, supporting the value of further development of this convenient chemotherapy-free regimen for patients with EGFR-positive advanced NSCLC who progressed after EGFR TKI therapy. Trial Registration: ChiCTR1900026273.
期刊介绍:
Signal Transduction and Targeted Therapy is an open access journal that focuses on timely publication of cutting-edge discoveries and advancements in basic science and clinical research related to signal transduction and targeted therapy.
Scope: The journal covers research on major human diseases, including, but not limited to:
Cancer,Cardiovascular diseases,Autoimmune diseases,Nervous system diseases.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
