Congcong Ma, Xiaoyu Long, Liying Yan, Xiaohui Zhu, Lixue Chen, Rong Li, Ying Wang, Jie Qiao
{"title":"卵巢刺激对胚胎非整倍体的影响:对 12 874 个卵母细胞和 3106 个囊胚进行的分析,这些卵母细胞和囊胚都进行了单基因遗传病植入前基因检测。","authors":"Congcong Ma, Xiaoyu Long, Liying Yan, Xiaohui Zhu, Lixue Chen, Rong Li, Ying Wang, Jie Qiao","doi":"10.1093/hropen/hoae054","DOIUrl":null,"url":null,"abstract":"<p><strong>Study question: </strong>Does ovarian stimulation and the ovarian response affect embryo euploidy?</p><p><strong>Summary answer: </strong>Ovarian stimulation and the ovarian response in women undergoing preimplantation genetic testing for monogenic disorders (PGT-M) cycles did not affect the rates of blastocyst euploidy.</p><p><strong>What is known already: </strong>Whether or not ovarian stimulation in IVF-embryo transfer has potential effects on embryo euploidy is controversial among studies for several reasons: (i) heterogeneity of the study populations, (ii) biopsies being performed at different stages of embryo development and (iii) evolution of the platforms utilized for ploidy assessment. Patients who undergo PGT-M cycles typically have no additional risks of aneuploidy, providing an ideal study population for exploring this issue.</p><p><strong>Study design size duration: </strong>A retrospective cohort study including embryos undergoing PGT-M was conducted at a single academically affiliated fertility clinic between June 2014 and July 2021.</p><p><strong>Participants/materials setting methods: </strong>A total of 617 women with 867 PGT-M cycles involving 12 874 retrieved oocytes and 3106 trophectoderm biopsies of blastocysts were included. The primary outcome of the study was median euploidy rate, which was calculated by dividing the number of euploid blastocysts by the total number of biopsied blastocysts for each cycle. Secondary outcomes included the median normal fertilization rate (two-pronuclear (2PN) embryos/metaphase II oocytes) and median blastulation rate (blastocyst numbers/2PN embryos).</p><p><strong>Main results and the role of chance: </strong>Comparable euploidy rates and fertilization rates were observed across all age groups, regardless of variations in ovarian stimulation protocols, gonadotropin dosages (both the starting and total dosages), stimulation durations, the inclusion of human menopausal gonadotrophin supplementation, or the number of oocytes retrieved (all <i>P</i> > 0.05). Blastulation rates declined with increasing starting doses of gonadotropins in women aged 31-34 years old (<i>P</i> = 0.005) but increased with increasing gonadotrophin starting doses in women aged 35-37 years old (<i>P</i> = 0.017). In women aged 31-34, 35-37, and 38-40 years old, blastulation rates were significantly reduced with increases in the number of oocytes retrieved (<i>P</i> = 0.001, <0.001, and 0.012, respectively).</p><p><strong>Limitations reasons for caution: </strong>Limitations include the study's retrospective nature and the relatively small number of patients of advanced age, especially patients older than 40 years old, leading to quite low statistical power. Second, as we considered euploidy rates as outcome measures, we did not analyze the effects of ovarian stimulation on uniform aneuploidy and mosaicism, respectively. Finally, we did not consider the effects of paternal characteristics on embryo euploidy status due to the fact that blastocyst aneuploidy primarily originates from maternal meiosis. However, sperm factors might have an effect on embryo development and the blastulation rate, and therefore also the number of blastocysts analyzed. The exclusion of patients with severe teratozoospermia and the fact that only ICSI was used as the insemination technique for women undergoing PGT-M contributed to minimize the effect of paternal factors.</p><p><strong>Wider implications of the findings: </strong>Ovarian stimulation and response to stimulation did not affect blastocyst euploidy rates in women undergoing PGT-M cycles. However, in women aged 31-40 years old, there was a significant decline in blastulation rates as the number of retrieved oocytes increased.</p><p><strong>Study funding/competing interests: </strong>This study was supported by the National Natural Science Foundation of China (Grant No. 81701407, 82301826); the National Key Research and Development Program of China (2022YFC2702901, 2022YFC2703004); China Postdoctoral Science Foundation (2022M710261), and China Postdoctoral Innovation Talent Support Program (BX20220020). There is no conflict of interest.</p><p><strong>Trial registration number: </strong>N/A.</p>","PeriodicalId":73264,"journal":{"name":"Human reproduction open","volume":"2024 4","pages":"hoae054"},"PeriodicalIF":11.1000,"publicationDate":"2024-10-03","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11470209/pdf/","citationCount":"0","resultStr":"{\"title\":\"Effects of ovarian stimulation on embryo euploidy: an analysis of 12 874 oocytes and 3106 blastocysts in cycles with preimplantation genetic testing for monogenic disorders.\",\"authors\":\"Congcong Ma, Xiaoyu Long, Liying Yan, Xiaohui Zhu, Lixue Chen, Rong Li, Ying Wang, Jie Qiao\",\"doi\":\"10.1093/hropen/hoae054\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Study question: </strong>Does ovarian stimulation and the ovarian response affect embryo euploidy?</p><p><strong>Summary answer: </strong>Ovarian stimulation and the ovarian response in women undergoing preimplantation genetic testing for monogenic disorders (PGT-M) cycles did not affect the rates of blastocyst euploidy.</p><p><strong>What is known already: </strong>Whether or not ovarian stimulation in IVF-embryo transfer has potential effects on embryo euploidy is controversial among studies for several reasons: (i) heterogeneity of the study populations, (ii) biopsies being performed at different stages of embryo development and (iii) evolution of the platforms utilized for ploidy assessment. Patients who undergo PGT-M cycles typically have no additional risks of aneuploidy, providing an ideal study population for exploring this issue.</p><p><strong>Study design size duration: </strong>A retrospective cohort study including embryos undergoing PGT-M was conducted at a single academically affiliated fertility clinic between June 2014 and July 2021.</p><p><strong>Participants/materials setting methods: </strong>A total of 617 women with 867 PGT-M cycles involving 12 874 retrieved oocytes and 3106 trophectoderm biopsies of blastocysts were included. The primary outcome of the study was median euploidy rate, which was calculated by dividing the number of euploid blastocysts by the total number of biopsied blastocysts for each cycle. Secondary outcomes included the median normal fertilization rate (two-pronuclear (2PN) embryos/metaphase II oocytes) and median blastulation rate (blastocyst numbers/2PN embryos).</p><p><strong>Main results and the role of chance: </strong>Comparable euploidy rates and fertilization rates were observed across all age groups, regardless of variations in ovarian stimulation protocols, gonadotropin dosages (both the starting and total dosages), stimulation durations, the inclusion of human menopausal gonadotrophin supplementation, or the number of oocytes retrieved (all <i>P</i> > 0.05). Blastulation rates declined with increasing starting doses of gonadotropins in women aged 31-34 years old (<i>P</i> = 0.005) but increased with increasing gonadotrophin starting doses in women aged 35-37 years old (<i>P</i> = 0.017). In women aged 31-34, 35-37, and 38-40 years old, blastulation rates were significantly reduced with increases in the number of oocytes retrieved (<i>P</i> = 0.001, <0.001, and 0.012, respectively).</p><p><strong>Limitations reasons for caution: </strong>Limitations include the study's retrospective nature and the relatively small number of patients of advanced age, especially patients older than 40 years old, leading to quite low statistical power. Second, as we considered euploidy rates as outcome measures, we did not analyze the effects of ovarian stimulation on uniform aneuploidy and mosaicism, respectively. Finally, we did not consider the effects of paternal characteristics on embryo euploidy status due to the fact that blastocyst aneuploidy primarily originates from maternal meiosis. However, sperm factors might have an effect on embryo development and the blastulation rate, and therefore also the number of blastocysts analyzed. The exclusion of patients with severe teratozoospermia and the fact that only ICSI was used as the insemination technique for women undergoing PGT-M contributed to minimize the effect of paternal factors.</p><p><strong>Wider implications of the findings: </strong>Ovarian stimulation and response to stimulation did not affect blastocyst euploidy rates in women undergoing PGT-M cycles. However, in women aged 31-40 years old, there was a significant decline in blastulation rates as the number of retrieved oocytes increased.</p><p><strong>Study funding/competing interests: </strong>This study was supported by the National Natural Science Foundation of China (Grant No. 81701407, 82301826); the National Key Research and Development Program of China (2022YFC2702901, 2022YFC2703004); China Postdoctoral Science Foundation (2022M710261), and China Postdoctoral Innovation Talent Support Program (BX20220020). There is no conflict of interest.</p><p><strong>Trial registration number: </strong>N/A.</p>\",\"PeriodicalId\":73264,\"journal\":{\"name\":\"Human reproduction open\",\"volume\":\"2024 4\",\"pages\":\"hoae054\"},\"PeriodicalIF\":11.1000,\"publicationDate\":\"2024-10-03\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11470209/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Human reproduction open\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1093/hropen/hoae054\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q1\",\"JCRName\":\"OBSTETRICS & GYNECOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Human reproduction open","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1093/hropen/hoae054","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/1/1 0:00:00","PubModel":"eCollection","JCR":"Q1","JCRName":"OBSTETRICS & GYNECOLOGY","Score":null,"Total":0}
Effects of ovarian stimulation on embryo euploidy: an analysis of 12 874 oocytes and 3106 blastocysts in cycles with preimplantation genetic testing for monogenic disorders.
Study question: Does ovarian stimulation and the ovarian response affect embryo euploidy?
Summary answer: Ovarian stimulation and the ovarian response in women undergoing preimplantation genetic testing for monogenic disorders (PGT-M) cycles did not affect the rates of blastocyst euploidy.
What is known already: Whether or not ovarian stimulation in IVF-embryo transfer has potential effects on embryo euploidy is controversial among studies for several reasons: (i) heterogeneity of the study populations, (ii) biopsies being performed at different stages of embryo development and (iii) evolution of the platforms utilized for ploidy assessment. Patients who undergo PGT-M cycles typically have no additional risks of aneuploidy, providing an ideal study population for exploring this issue.
Study design size duration: A retrospective cohort study including embryos undergoing PGT-M was conducted at a single academically affiliated fertility clinic between June 2014 and July 2021.
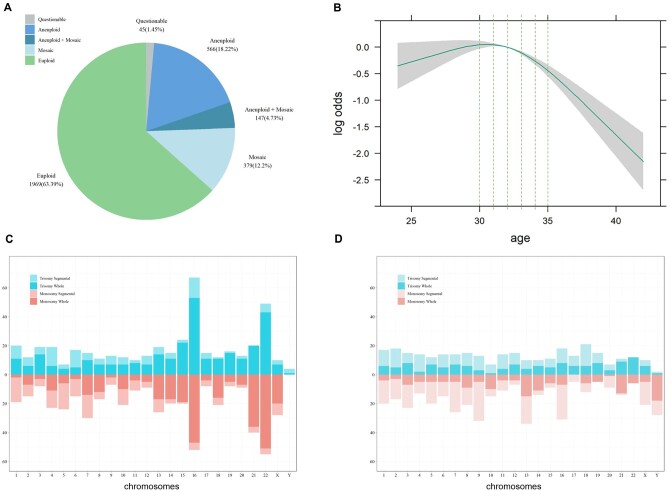
Participants/materials setting methods: A total of 617 women with 867 PGT-M cycles involving 12 874 retrieved oocytes and 3106 trophectoderm biopsies of blastocysts were included. The primary outcome of the study was median euploidy rate, which was calculated by dividing the number of euploid blastocysts by the total number of biopsied blastocysts for each cycle. Secondary outcomes included the median normal fertilization rate (two-pronuclear (2PN) embryos/metaphase II oocytes) and median blastulation rate (blastocyst numbers/2PN embryos).
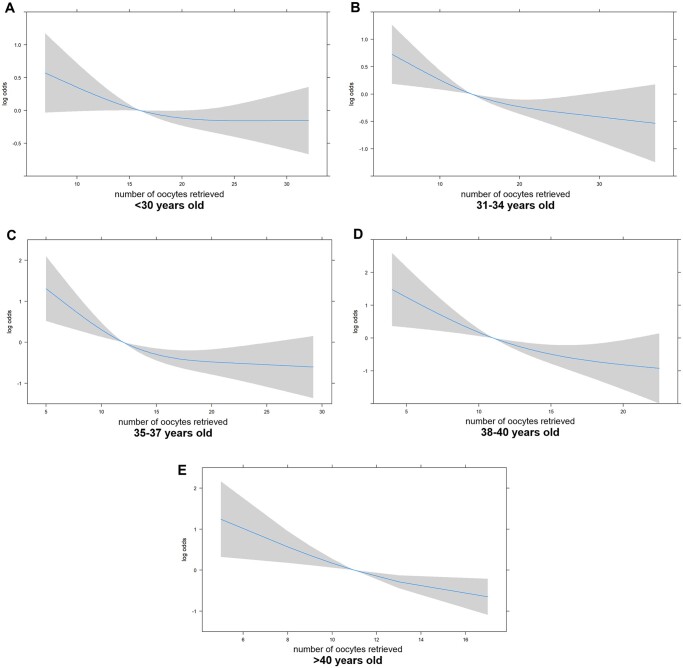
Main results and the role of chance: Comparable euploidy rates and fertilization rates were observed across all age groups, regardless of variations in ovarian stimulation protocols, gonadotropin dosages (both the starting and total dosages), stimulation durations, the inclusion of human menopausal gonadotrophin supplementation, or the number of oocytes retrieved (all P > 0.05). Blastulation rates declined with increasing starting doses of gonadotropins in women aged 31-34 years old (P = 0.005) but increased with increasing gonadotrophin starting doses in women aged 35-37 years old (P = 0.017). In women aged 31-34, 35-37, and 38-40 years old, blastulation rates were significantly reduced with increases in the number of oocytes retrieved (P = 0.001, <0.001, and 0.012, respectively).
Limitations reasons for caution: Limitations include the study's retrospective nature and the relatively small number of patients of advanced age, especially patients older than 40 years old, leading to quite low statistical power. Second, as we considered euploidy rates as outcome measures, we did not analyze the effects of ovarian stimulation on uniform aneuploidy and mosaicism, respectively. Finally, we did not consider the effects of paternal characteristics on embryo euploidy status due to the fact that blastocyst aneuploidy primarily originates from maternal meiosis. However, sperm factors might have an effect on embryo development and the blastulation rate, and therefore also the number of blastocysts analyzed. The exclusion of patients with severe teratozoospermia and the fact that only ICSI was used as the insemination technique for women undergoing PGT-M contributed to minimize the effect of paternal factors.
Wider implications of the findings: Ovarian stimulation and response to stimulation did not affect blastocyst euploidy rates in women undergoing PGT-M cycles. However, in women aged 31-40 years old, there was a significant decline in blastulation rates as the number of retrieved oocytes increased.
Study funding/competing interests: This study was supported by the National Natural Science Foundation of China (Grant No. 81701407, 82301826); the National Key Research and Development Program of China (2022YFC2702901, 2022YFC2703004); China Postdoctoral Science Foundation (2022M710261), and China Postdoctoral Innovation Talent Support Program (BX20220020). There is no conflict of interest.



 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
