Yingxue Li, Jeroen V Koomen, Douglas J Eleveld, Johannes P van den Berg, Jaap Jan Vos, Ilonka N de Keijzer, Michel M R F Struys, Pieter J Colin
{"title":"全身麻醉前和麻醉过程中健康志愿者体内去甲肾上腺素的群体药代动力学模型。","authors":"Yingxue Li, Jeroen V Koomen, Douglas J Eleveld, Johannes P van den Berg, Jaap Jan Vos, Ilonka N de Keijzer, Michel M R F Struys, Pieter J Colin","doi":"10.1007/s40262-024-01430-y","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Intraoperation hypotension (IOH) is commonly observed in patients undergoing surgery under general anesthesia, and even a brief episode of IOH can lead to unfavorable outcomes. To reduce the risk, blood pressure is closely measured during general anesthesia, and norepinephrine (NE) is frequently administered if hypotension is detected. Despite its routine application, information on the dose-exposure-response relationship of NE remains limited. Additionally, quantification of the influence of general anesthesia on the pharmacokinetics (PK) of NE is lacking.</p><p><strong>Objective: </strong>In this study, we aimed to describe NE PK in healthy volunteers and the influence of general anesthesia on its PK.</p><p><strong>Methods: </strong>A single-center, cross-over study was conducted in healthy volunteers. The volunteers received a step-up NE dosing scheme (0.04, 0.08, 0.12, 0.16 and 0.20 mcg<sup>-1</sup>/kg<sup>-1</sup>/min<sup>-1</sup>) first in the awake state and then under general anesthesia. General anesthesia was administered using a propofol/remifentanil Eleveld target-controlled infusion. During general anesthesia, a 30-second electrical stimulus was given as surrogate for surgical incision to the volunteers at each dosage step. Blood samples were drawn before the initial dosing and after each dosing step, and plasma NE, propofol and remifentanil concentrations were subsequently determined. A population PK model was developed using non-linear mixed effects modelling. Simulations were conducted to predict the plasma NE concentration in patients at different measured propofol concentrations.</p><p><strong>Results: </strong>A total of 1219 samples were analyzed from 36 volunteers. A two-compartment model with a first-order elimination best described the data. Weight, age, and session effect (awake vs general anesthesia) were identified as relevant covariates on the clearance (CL) of NE. A 10% decrease in NE CL was observed after general anesthesia induction. This difference between sessions is better explained by the measured concentration of propofol, rather than the anticipated impact of cardiac output. The estimated post-stimulation NE concentration is 0.66 nmol/L<sup>-1</sup> (95% CI 0.06-1.20 nmol/L<sup>-1</sup>) lower than the pre-stimulation NE concentration. Model simulation indicates that patients at a higher measured propofol concentration (e.g., 6 mcg/mL<sup>-1</sup>) exhibited higher NE concentrations (95% PI 18.10-43.89 nmol/L<sup>-1</sup>) than patients at a lower measured propofol concentration (e.g., 3 mcg/mL<sup>-1</sup>) (95% PI 16.81-38.91 nmol L<sup>-1</sup>).</p><p><strong>Conclusion: </strong>The NE PK is well described with a two-compartment model with a first-order elimination. NE CL exhibiting a 10% decrease under general anesthesia, with this difference being attributed to the measured concentration of propofol. The impact of stimulation on NE PK under general anesthesia is very limited.</p><p><strong>Clinical trials registration number: </strong>NL9312.</p>","PeriodicalId":10405,"journal":{"name":"Clinical Pharmacokinetics","volume":" ","pages":"1597-1608"},"PeriodicalIF":4.0000,"publicationDate":"2024-11-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11573843/pdf/","citationCount":"0","resultStr":"{\"title\":\"Population Pharmacokinetic Modelling of Norepinephrine in Healthy Volunteers Prior to and During General Anesthesia.\",\"authors\":\"Yingxue Li, Jeroen V Koomen, Douglas J Eleveld, Johannes P van den Berg, Jaap Jan Vos, Ilonka N de Keijzer, Michel M R F Struys, Pieter J Colin\",\"doi\":\"10.1007/s40262-024-01430-y\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Intraoperation hypotension (IOH) is commonly observed in patients undergoing surgery under general anesthesia, and even a brief episode of IOH can lead to unfavorable outcomes. To reduce the risk, blood pressure is closely measured during general anesthesia, and norepinephrine (NE) is frequently administered if hypotension is detected. Despite its routine application, information on the dose-exposure-response relationship of NE remains limited. Additionally, quantification of the influence of general anesthesia on the pharmacokinetics (PK) of NE is lacking.</p><p><strong>Objective: </strong>In this study, we aimed to describe NE PK in healthy volunteers and the influence of general anesthesia on its PK.</p><p><strong>Methods: </strong>A single-center, cross-over study was conducted in healthy volunteers. The volunteers received a step-up NE dosing scheme (0.04, 0.08, 0.12, 0.16 and 0.20 mcg<sup>-1</sup>/kg<sup>-1</sup>/min<sup>-1</sup>) first in the awake state and then under general anesthesia. General anesthesia was administered using a propofol/remifentanil Eleveld target-controlled infusion. During general anesthesia, a 30-second electrical stimulus was given as surrogate for surgical incision to the volunteers at each dosage step. Blood samples were drawn before the initial dosing and after each dosing step, and plasma NE, propofol and remifentanil concentrations were subsequently determined. A population PK model was developed using non-linear mixed effects modelling. Simulations were conducted to predict the plasma NE concentration in patients at different measured propofol concentrations.</p><p><strong>Results: </strong>A total of 1219 samples were analyzed from 36 volunteers. A two-compartment model with a first-order elimination best described the data. Weight, age, and session effect (awake vs general anesthesia) were identified as relevant covariates on the clearance (CL) of NE. A 10% decrease in NE CL was observed after general anesthesia induction. This difference between sessions is better explained by the measured concentration of propofol, rather than the anticipated impact of cardiac output. The estimated post-stimulation NE concentration is 0.66 nmol/L<sup>-1</sup> (95% CI 0.06-1.20 nmol/L<sup>-1</sup>) lower than the pre-stimulation NE concentration. Model simulation indicates that patients at a higher measured propofol concentration (e.g., 6 mcg/mL<sup>-1</sup>) exhibited higher NE concentrations (95% PI 18.10-43.89 nmol/L<sup>-1</sup>) than patients at a lower measured propofol concentration (e.g., 3 mcg/mL<sup>-1</sup>) (95% PI 16.81-38.91 nmol L<sup>-1</sup>).</p><p><strong>Conclusion: </strong>The NE PK is well described with a two-compartment model with a first-order elimination. NE CL exhibiting a 10% decrease under general anesthesia, with this difference being attributed to the measured concentration of propofol. The impact of stimulation on NE PK under general anesthesia is very limited.</p><p><strong>Clinical trials registration number: </strong>NL9312.</p>\",\"PeriodicalId\":10405,\"journal\":{\"name\":\"Clinical Pharmacokinetics\",\"volume\":\" \",\"pages\":\"1597-1608\"},\"PeriodicalIF\":4.0000,\"publicationDate\":\"2024-11-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11573843/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Clinical Pharmacokinetics\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1007/s40262-024-01430-y\",\"RegionNum\":2,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/10/27 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q1\",\"JCRName\":\"PHARMACOLOGY & PHARMACY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Clinical Pharmacokinetics","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1007/s40262-024-01430-y","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/10/27 0:00:00","PubModel":"Epub","JCR":"Q1","JCRName":"PHARMACOLOGY & PHARMACY","Score":null,"Total":0}
引用次数: 0
摘要
背景:在全身麻醉下接受手术的患者通常会出现术中低血压(IOH),即使是短暂的术中低血压发作也会导致不良后果。为了降低风险,在全身麻醉期间要密切测量血压,如果发现低血压,则要经常使用去甲肾上腺素(NE)。尽管 NE 已被常规应用,但有关其剂量-暴露-反应关系的信息仍然有限。此外,关于全身麻醉对去甲肾上腺素药代动力学(PK)影响的量化研究也很缺乏:本研究旨在描述健康志愿者体内 NE 的 PK 值以及全身麻醉对其 PK 值的影响:方法:在健康志愿者中开展了一项单中心、交叉研究。志愿者首先在清醒状态下,然后在全身麻醉状态下接受阶梯式 NE 给药方案(0.04、0.08、0.12、0.16 和 0.20 mcg-1/kg-1/min-1)。全身麻醉采用异丙酚/瑞芬太尼Eleveld靶控输注法。在全身麻醉期间,志愿者在每个剂量阶段都会受到 30 秒钟的电刺激,以替代手术切口。在首次给药前和每次给药后抽取血样,随后测定血浆中NE、丙泊酚和瑞芬太尼的浓度。采用非线性混合效应模型建立了群体 PK 模型。模拟预测了不同丙泊酚测量浓度下患者的血浆NE浓度:结果:共分析了来自 36 名志愿者的 1219 份样本。采用一阶消除的二室模型对数据进行了最佳描述。体重、年龄和疗程效应(清醒与全身麻醉)被确定为 NE 清除率(CL)的相关协变量。在全身麻醉诱导后观察到 NE 的清除率降低了 10%。与预期的心输出量的影响相比,异丙酚的测定浓度更能解释疗程间的这种差异。估计的刺激后 NE 浓度比刺激前 NE 浓度低 0.66 nmol/L-1(95% CI 0.06-1.20 nmol/L-1)。模型模拟表明,丙泊酚测量浓度较高的患者(如 6 mcg/mL-1)的 NE 浓度(95% PI 18.10-43.89 nmol/L-1)高于丙泊酚测量浓度较低的患者(如 3 mcg/mL-1)(95% PI 16.81-38.91 nmol L-1):结论:采用一阶消除的二室模型可以很好地描述 NE 的 PK 值。在全身麻醉状态下,NE的CL值下降了10%,这种差异是由于丙泊酚的测量浓度造成的。在全身麻醉状态下,刺激对NE PK的影响非常有限:临床试验注册号:NL9312。
Population Pharmacokinetic Modelling of Norepinephrine in Healthy Volunteers Prior to and During General Anesthesia.
Background: Intraoperation hypotension (IOH) is commonly observed in patients undergoing surgery under general anesthesia, and even a brief episode of IOH can lead to unfavorable outcomes. To reduce the risk, blood pressure is closely measured during general anesthesia, and norepinephrine (NE) is frequently administered if hypotension is detected. Despite its routine application, information on the dose-exposure-response relationship of NE remains limited. Additionally, quantification of the influence of general anesthesia on the pharmacokinetics (PK) of NE is lacking.
Objective: In this study, we aimed to describe NE PK in healthy volunteers and the influence of general anesthesia on its PK.
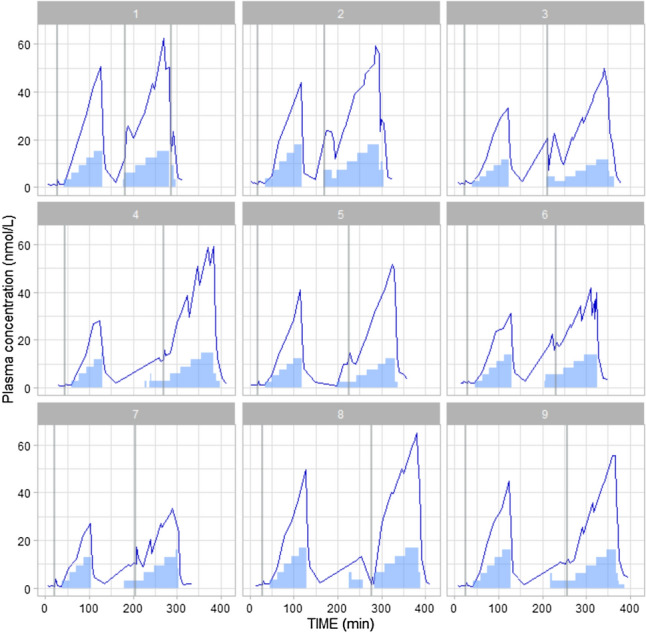
Methods: A single-center, cross-over study was conducted in healthy volunteers. The volunteers received a step-up NE dosing scheme (0.04, 0.08, 0.12, 0.16 and 0.20 mcg-1/kg-1/min-1) first in the awake state and then under general anesthesia. General anesthesia was administered using a propofol/remifentanil Eleveld target-controlled infusion. During general anesthesia, a 30-second electrical stimulus was given as surrogate for surgical incision to the volunteers at each dosage step. Blood samples were drawn before the initial dosing and after each dosing step, and plasma NE, propofol and remifentanil concentrations were subsequently determined. A population PK model was developed using non-linear mixed effects modelling. Simulations were conducted to predict the plasma NE concentration in patients at different measured propofol concentrations.
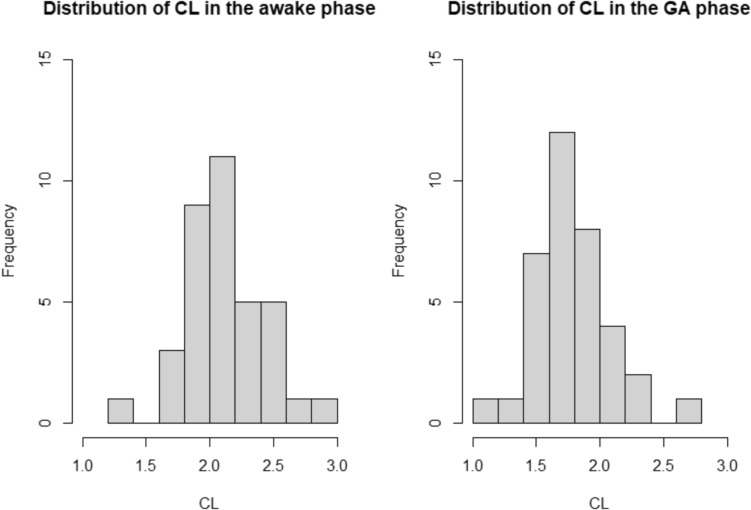
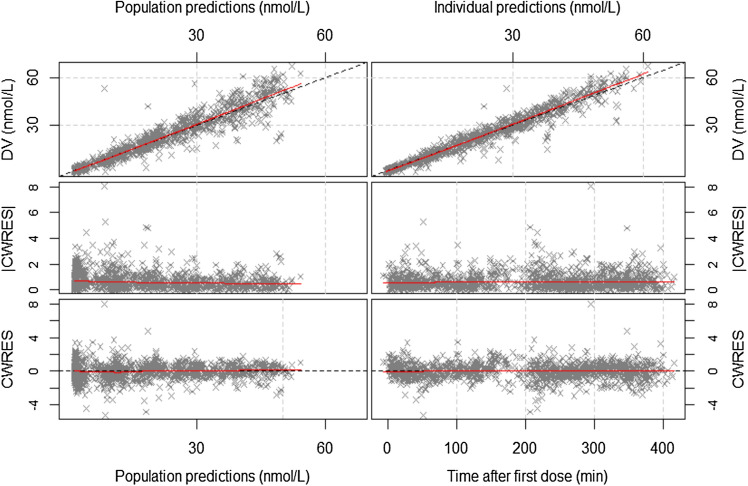
Results: A total of 1219 samples were analyzed from 36 volunteers. A two-compartment model with a first-order elimination best described the data. Weight, age, and session effect (awake vs general anesthesia) were identified as relevant covariates on the clearance (CL) of NE. A 10% decrease in NE CL was observed after general anesthesia induction. This difference between sessions is better explained by the measured concentration of propofol, rather than the anticipated impact of cardiac output. The estimated post-stimulation NE concentration is 0.66 nmol/L-1 (95% CI 0.06-1.20 nmol/L-1) lower than the pre-stimulation NE concentration. Model simulation indicates that patients at a higher measured propofol concentration (e.g., 6 mcg/mL-1) exhibited higher NE concentrations (95% PI 18.10-43.89 nmol/L-1) than patients at a lower measured propofol concentration (e.g., 3 mcg/mL-1) (95% PI 16.81-38.91 nmol L-1).
Conclusion: The NE PK is well described with a two-compartment model with a first-order elimination. NE CL exhibiting a 10% decrease under general anesthesia, with this difference being attributed to the measured concentration of propofol. The impact of stimulation on NE PK under general anesthesia is very limited.
期刊介绍:
Clinical Pharmacokinetics promotes the continuing development of clinical pharmacokinetics and pharmacodynamics for the improvement of drug therapy, and for furthering postgraduate education in clinical pharmacology and therapeutics.
Pharmacokinetics, the study of drug disposition in the body, is an integral part of drug development and rational use. Knowledge and application of pharmacokinetic principles leads to accelerated drug development, cost effective drug use and a reduced frequency of adverse effects and drug interactions.



 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
