Kevin Louie, Shaili Amatya, Gad Alpan, Lance A Parton
{"title":"使用神经调节通气辅助系统(NAVA)进行无创通气可改善极低出生体重儿的拔管效果。","authors":"Kevin Louie, Shaili Amatya, Gad Alpan, Lance A Parton","doi":"10.3390/children11101184","DOIUrl":null,"url":null,"abstract":"<p><p><b>Objective:</b> This study investigates the effectiveness of extubation from conventional mechanical ventilation using an endotracheal tube (MVET) compared to synchronized non-invasive positive-pressure ventilation (sNIPPV) using neurally adjusted ventilatory assist (NAVA) and conventional non-invasive positive-pressure ventilation (NIPPV) in extremely low-birth-weight (ELBW) infants. <b>Methods:</b> An institutional review board (IRB) approved this study (#12175) to conduct a single-center randomized control trial including 60 ELBW infants assigned in a one-to-one computer-generated scheme to either sNIPPV using NAVA or NIPPV. The primary outcome involved the need for reintubation, and the secondary outcome involved the assessment of moderate/severe BPD, defined as an oxygen requirement at 36 weeks, as in #NCT03613987 (clinicaltrials.gov). <b>Results:</b> There were 60 ELBW infants enrolled and randomized. The overall gestational age was 26 (1.5) weeks, and the birth weight was 773 (157) g [mean (SD)]. There were no statistically significant differences between the NAVA and NIPPV patient characteristics. There was a 41% extubation failure rate in the NIPPV group and 35% in the NAVA group (<i>p</i> = NS). The NAVA group had less moderate and severe BPD (<i>p</i> = 0.03), a shorter oxygen therapy duration (<i>p</i> = 0.002), a decreased length of stay (<i>p</i> = 0.03), and less need for home oxygen (0, 43%; <i>p</i> = 0.0004). <b>Conclusions:</b> This study found similar extubation failure rates among ELBW infants as in prior studies. However, the NAVA group had lower rates of moderate/severe BPD and need for oxygen at discharge, as well as shorter oxygen therapy duration and length of stay. The use of NAVA may be a reasonable alternative mode of non-invasive ventilation in the ELBW population.</p>","PeriodicalId":48588,"journal":{"name":"Children-Basel","volume":"11 10","pages":""},"PeriodicalIF":2.6000,"publicationDate":"2024-09-28","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11506030/pdf/","citationCount":"0","resultStr":"{\"title\":\"Non-Invasive Ventilation with Neurally Adjusted Ventilatory Assist (NAVA) Improves Extubation Outcomes in Extremely Low-Birth-Weight Infants.\",\"authors\":\"Kevin Louie, Shaili Amatya, Gad Alpan, Lance A Parton\",\"doi\":\"10.3390/children11101184\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p><b>Objective:</b> This study investigates the effectiveness of extubation from conventional mechanical ventilation using an endotracheal tube (MVET) compared to synchronized non-invasive positive-pressure ventilation (sNIPPV) using neurally adjusted ventilatory assist (NAVA) and conventional non-invasive positive-pressure ventilation (NIPPV) in extremely low-birth-weight (ELBW) infants. <b>Methods:</b> An institutional review board (IRB) approved this study (#12175) to conduct a single-center randomized control trial including 60 ELBW infants assigned in a one-to-one computer-generated scheme to either sNIPPV using NAVA or NIPPV. The primary outcome involved the need for reintubation, and the secondary outcome involved the assessment of moderate/severe BPD, defined as an oxygen requirement at 36 weeks, as in #NCT03613987 (clinicaltrials.gov). <b>Results:</b> There were 60 ELBW infants enrolled and randomized. The overall gestational age was 26 (1.5) weeks, and the birth weight was 773 (157) g [mean (SD)]. There were no statistically significant differences between the NAVA and NIPPV patient characteristics. There was a 41% extubation failure rate in the NIPPV group and 35% in the NAVA group (<i>p</i> = NS). The NAVA group had less moderate and severe BPD (<i>p</i> = 0.03), a shorter oxygen therapy duration (<i>p</i> = 0.002), a decreased length of stay (<i>p</i> = 0.03), and less need for home oxygen (0, 43%; <i>p</i> = 0.0004). <b>Conclusions:</b> This study found similar extubation failure rates among ELBW infants as in prior studies. However, the NAVA group had lower rates of moderate/severe BPD and need for oxygen at discharge, as well as shorter oxygen therapy duration and length of stay. The use of NAVA may be a reasonable alternative mode of non-invasive ventilation in the ELBW population.</p>\",\"PeriodicalId\":48588,\"journal\":{\"name\":\"Children-Basel\",\"volume\":\"11 10\",\"pages\":\"\"},\"PeriodicalIF\":2.6000,\"publicationDate\":\"2024-09-28\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11506030/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Children-Basel\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.3390/children11101184\",\"RegionNum\":4,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"PEDIATRICS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Children-Basel","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.3390/children11101184","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"PEDIATRICS","Score":null,"Total":0}
Non-Invasive Ventilation with Neurally Adjusted Ventilatory Assist (NAVA) Improves Extubation Outcomes in Extremely Low-Birth-Weight Infants.
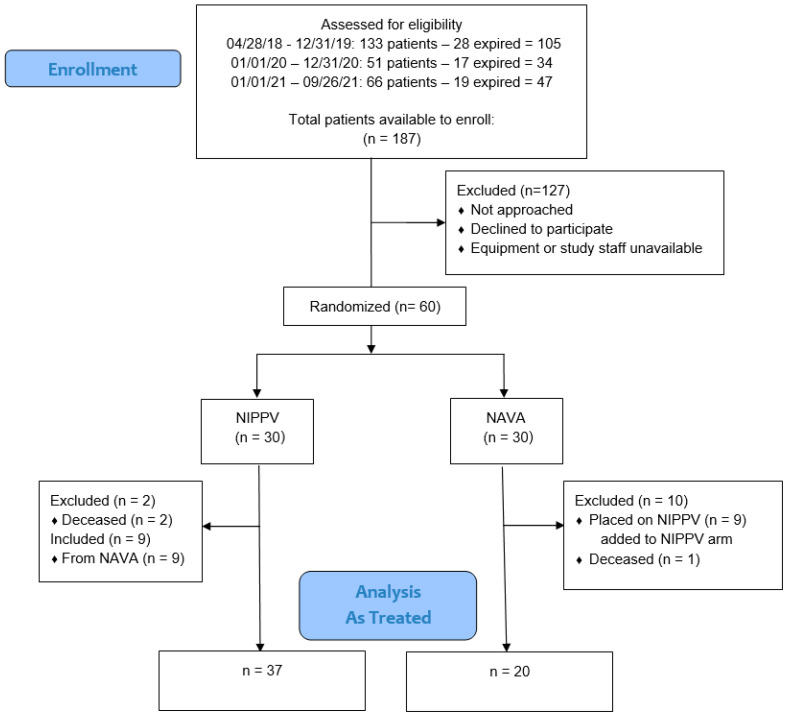
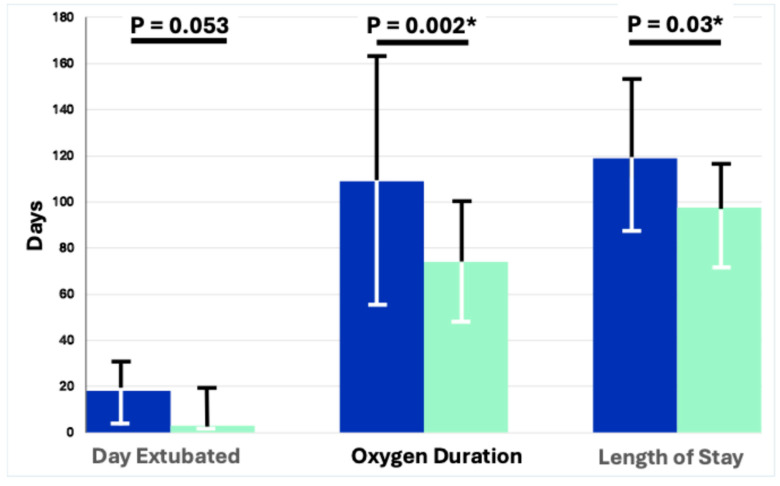
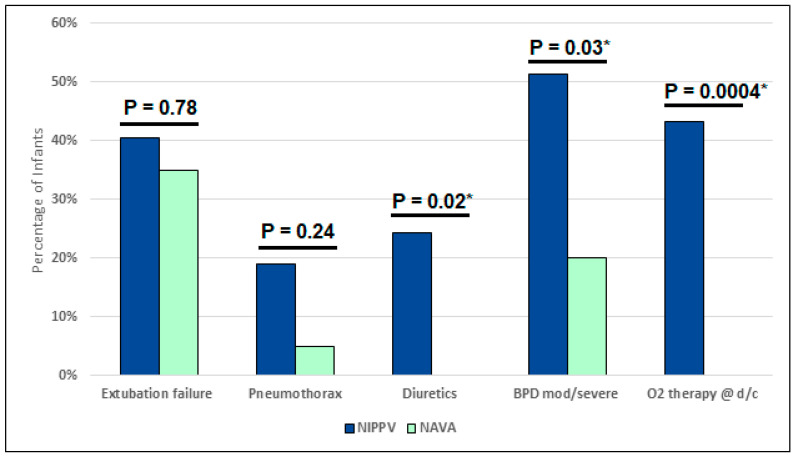
Objective: This study investigates the effectiveness of extubation from conventional mechanical ventilation using an endotracheal tube (MVET) compared to synchronized non-invasive positive-pressure ventilation (sNIPPV) using neurally adjusted ventilatory assist (NAVA) and conventional non-invasive positive-pressure ventilation (NIPPV) in extremely low-birth-weight (ELBW) infants. Methods: An institutional review board (IRB) approved this study (#12175) to conduct a single-center randomized control trial including 60 ELBW infants assigned in a one-to-one computer-generated scheme to either sNIPPV using NAVA or NIPPV. The primary outcome involved the need for reintubation, and the secondary outcome involved the assessment of moderate/severe BPD, defined as an oxygen requirement at 36 weeks, as in #NCT03613987 (clinicaltrials.gov). Results: There were 60 ELBW infants enrolled and randomized. The overall gestational age was 26 (1.5) weeks, and the birth weight was 773 (157) g [mean (SD)]. There were no statistically significant differences between the NAVA and NIPPV patient characteristics. There was a 41% extubation failure rate in the NIPPV group and 35% in the NAVA group (p = NS). The NAVA group had less moderate and severe BPD (p = 0.03), a shorter oxygen therapy duration (p = 0.002), a decreased length of stay (p = 0.03), and less need for home oxygen (0, 43%; p = 0.0004). Conclusions: This study found similar extubation failure rates among ELBW infants as in prior studies. However, the NAVA group had lower rates of moderate/severe BPD and need for oxygen at discharge, as well as shorter oxygen therapy duration and length of stay. The use of NAVA may be a reasonable alternative mode of non-invasive ventilation in the ELBW population.
期刊介绍:
Children is an international, open access journal dedicated to a streamlined, yet scientifically rigorous, dissemination of peer-reviewed science related to childhood health and disease in developed and developing countries.
The publication focuses on sharing clinical, epidemiological and translational science relevant to children’s health. Moreover, the primary goals of the publication are to highlight under‑represented pediatric disciplines, to emphasize interdisciplinary research and to disseminate advances in knowledge in global child health. In addition to original research, the journal publishes expert editorials and commentaries, clinical case reports, and insightful communications reflecting the latest developments in pediatric medicine. By publishing meritorious articles as soon as the editorial review process is completed, rather than at predefined intervals, Children also permits rapid open access sharing of new information, allowing us to reach the broadest audience in the most expedient fashion.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
