Jessica Ammon, John Alexander, Woodson Petit-Frere, Deya Alkhatib, Aranyak Rawal, Grace Newman, Oguz Akbiligic, Brian Borkowski, John Jefferies, Isaac B Rhea
{"title":"利用回顾性算法提高临床医生对 ATTR 淀粉样变性的怀疑。","authors":"Jessica Ammon, John Alexander, Woodson Petit-Frere, Deya Alkhatib, Aranyak Rawal, Grace Newman, Oguz Akbiligic, Brian Borkowski, John Jefferies, Isaac B Rhea","doi":"10.1186/s40959-024-00282-6","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>This study aimed to increase the index of suspicion for transthyretin amyloidosis (ATTR) among cardiologists leading to increased screening for amyloidosis.</p><p><strong>Methods: </strong>A retrospective algorithm was created to identify patients at risk for ATTR. A list of these patients and instructions on how to order amyloidosis testing were given to cardiologists, who then determined if further evaluation was warranted. The ordering trends of Technetium 99 m-Pyrophosphate (PYP) scans and the number of ordering physicians before and after this intervention were recorded across the entire practice.</p><p><strong>Results: </strong>The algorithm identified 349 potential high-risk patients of which only 23 eventually had PYP scans performed resulting in 2 equivocal and 1 positive results. Across the practice, over the 28 months before initiating this protocol, PYP scans were ordered for 22 patients of which 6 were equivocal or positive. Over the 23-month course of this project, 142 PYP scans were ordered of which 18 were equivocal or positive. The number of ordering providers increased from 7 prior to the protocol's implementation to 22 by the end of this project within 23 months. On change point analysis, PYP scan ordering increased after protocol initiation (regression coefficient 1.27 vs. 6.31, p < 0.001), as well as equivocal or positive PYP results (regression coefficient 0.38 vs. 0.52, p < 0.01).</p><p><strong>Conclusion: </strong>The results of this study suggest that using this algorithm, despite it not being independently predictive of ATTR, did result in our clinicians having a lower threshold for testing for ATTR. More clinicians ordered appropriate testing, and more positive tests were obtained.</p>","PeriodicalId":9804,"journal":{"name":"Cardio-oncology","volume":"10 1","pages":"78"},"PeriodicalIF":3.2000,"publicationDate":"2024-11-08","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11546096/pdf/","citationCount":"0","resultStr":"{\"title\":\"Increasing clinicians' suspicion of ATTR amyloidosis using a retrospective algorithm.\",\"authors\":\"Jessica Ammon, John Alexander, Woodson Petit-Frere, Deya Alkhatib, Aranyak Rawal, Grace Newman, Oguz Akbiligic, Brian Borkowski, John Jefferies, Isaac B Rhea\",\"doi\":\"10.1186/s40959-024-00282-6\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>This study aimed to increase the index of suspicion for transthyretin amyloidosis (ATTR) among cardiologists leading to increased screening for amyloidosis.</p><p><strong>Methods: </strong>A retrospective algorithm was created to identify patients at risk for ATTR. A list of these patients and instructions on how to order amyloidosis testing were given to cardiologists, who then determined if further evaluation was warranted. The ordering trends of Technetium 99 m-Pyrophosphate (PYP) scans and the number of ordering physicians before and after this intervention were recorded across the entire practice.</p><p><strong>Results: </strong>The algorithm identified 349 potential high-risk patients of which only 23 eventually had PYP scans performed resulting in 2 equivocal and 1 positive results. Across the practice, over the 28 months before initiating this protocol, PYP scans were ordered for 22 patients of which 6 were equivocal or positive. Over the 23-month course of this project, 142 PYP scans were ordered of which 18 were equivocal or positive. The number of ordering providers increased from 7 prior to the protocol's implementation to 22 by the end of this project within 23 months. On change point analysis, PYP scan ordering increased after protocol initiation (regression coefficient 1.27 vs. 6.31, p < 0.001), as well as equivocal or positive PYP results (regression coefficient 0.38 vs. 0.52, p < 0.01).</p><p><strong>Conclusion: </strong>The results of this study suggest that using this algorithm, despite it not being independently predictive of ATTR, did result in our clinicians having a lower threshold for testing for ATTR. More clinicians ordered appropriate testing, and more positive tests were obtained.</p>\",\"PeriodicalId\":9804,\"journal\":{\"name\":\"Cardio-oncology\",\"volume\":\"10 1\",\"pages\":\"78\"},\"PeriodicalIF\":3.2000,\"publicationDate\":\"2024-11-08\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11546096/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Cardio-oncology\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1186/s40959-024-00282-6\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"CARDIAC & CARDIOVASCULAR SYSTEMS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Cardio-oncology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1186/s40959-024-00282-6","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
Increasing clinicians' suspicion of ATTR amyloidosis using a retrospective algorithm.
Background: This study aimed to increase the index of suspicion for transthyretin amyloidosis (ATTR) among cardiologists leading to increased screening for amyloidosis.
Methods: A retrospective algorithm was created to identify patients at risk for ATTR. A list of these patients and instructions on how to order amyloidosis testing were given to cardiologists, who then determined if further evaluation was warranted. The ordering trends of Technetium 99 m-Pyrophosphate (PYP) scans and the number of ordering physicians before and after this intervention were recorded across the entire practice.
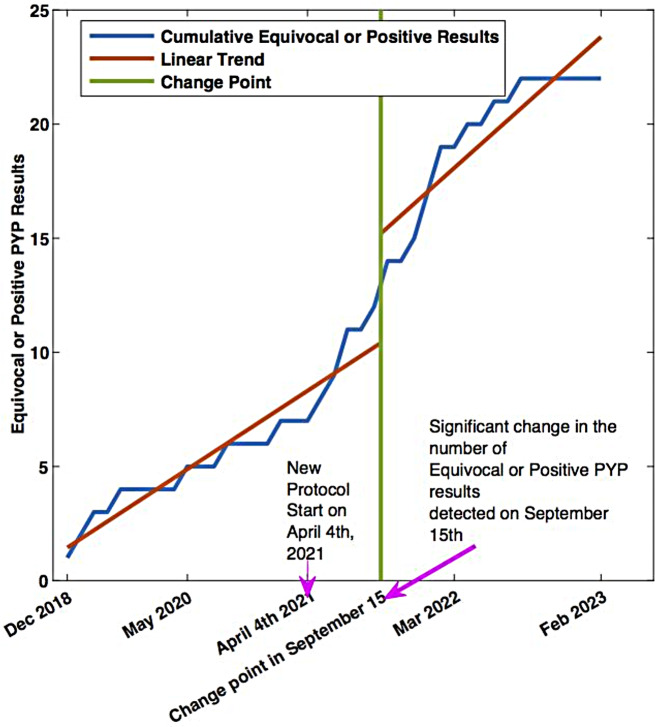
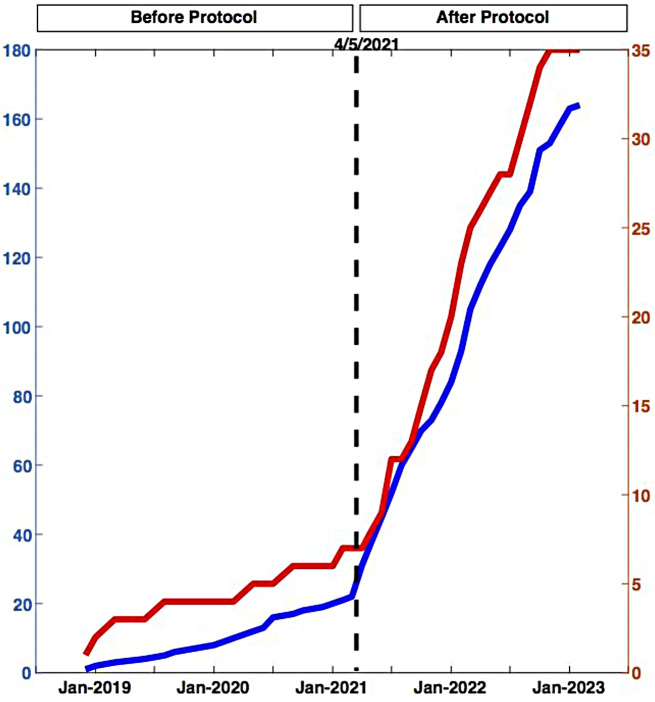
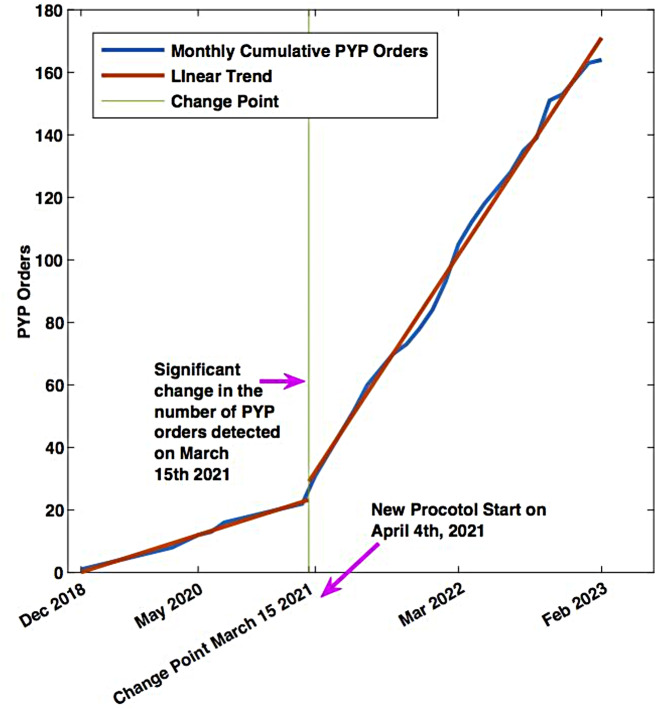
Results: The algorithm identified 349 potential high-risk patients of which only 23 eventually had PYP scans performed resulting in 2 equivocal and 1 positive results. Across the practice, over the 28 months before initiating this protocol, PYP scans were ordered for 22 patients of which 6 were equivocal or positive. Over the 23-month course of this project, 142 PYP scans were ordered of which 18 were equivocal or positive. The number of ordering providers increased from 7 prior to the protocol's implementation to 22 by the end of this project within 23 months. On change point analysis, PYP scan ordering increased after protocol initiation (regression coefficient 1.27 vs. 6.31, p < 0.001), as well as equivocal or positive PYP results (regression coefficient 0.38 vs. 0.52, p < 0.01).
Conclusion: The results of this study suggest that using this algorithm, despite it not being independently predictive of ATTR, did result in our clinicians having a lower threshold for testing for ATTR. More clinicians ordered appropriate testing, and more positive tests were obtained.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
