Geoffrey J. Hoffman PhD, Jinkyung Ha PhD, Zhaohui Fan MD, MPH, Jun Li PhD
{"title":"农村医院关闭与急性和急性后护理机会和结果之间的关系。","authors":"Geoffrey J. Hoffman PhD, Jinkyung Ha PhD, Zhaohui Fan MD, MPH, Jun Li PhD","doi":"10.1111/1475-6773.14426","DOIUrl":null,"url":null,"abstract":"<div>\n \n \n <section>\n \n <h3> Objective</h3>\n \n <p>To determine whether rural hospital closures affected hospital and post-acute care (PAC) use and outcomes.</p>\n </section>\n \n <section>\n \n <h3> Study Setting and Design</h3>\n \n <p>Using a staggered difference-in-differences design, we evaluated associations between 32 rural hospital closures and changes in county-level: (1) travel distances to and lengths of stay at hospitals; (2) functional limitations at and time from hospital discharge to start of PAC episode; (3) 30-day readmissions and mortality and hospitalizations for a fall-related injury; and (4) population-level hospitalization and death rates.</p>\n </section>\n \n <section>\n \n <h3> Data Sources and Analytic Sample</h3>\n \n <p>100% Medicare claims and home health and skilled nursing facility clinical data to identify approximately 3 million discharges for older fee-for-service Medicare beneficiaries.</p>\n </section>\n \n <section>\n \n <h3> Principal Findings</h3>\n \n <p>We found that hospitals that closed compared to those remaining open served more minoritized, lower-income populations, including more Medicaid and fewer commercial patients, and had lower profit margins. Following a closure, quarterly hospitalization rates (111.6 quarterly hospitalizations per 10,000 older adults; 95% CI: 53.4, 170.9) and average hospital lengths of stay increased (0.34 days; 95% CI: 0.13, 0.56 days). We observed no change in the average distance between patients' residential ZIP code and the hospital used (0.29 miles; 95% CI: −1.06, 1.64 miles); average number of standardized ADL limitations at PAC (0.08 SDs from the pre-closure average; 95% CI: −0.12, 0.28 SDs); or PAC time to start (0.02 days; 95% CI: −1.2, 1.2 days). Among more isolated hospitals, closures were associated with an increase in the likelihood of readmission (0.10 percentage-points; 95% CI: 0.00, 0.19).</p>\n </section>\n \n <section>\n \n <h3> Conclusions</h3>\n \n <p>Closures were not associated with notably worsened health care access, function, or health, potentially because closures triggered care delivery adjustments involving increased numbers of patients seeking out higher quality care.</p>\n </section>\n </div>","PeriodicalId":55065,"journal":{"name":"Health Services Research","volume":"60 3","pages":""},"PeriodicalIF":3.2000,"publicationDate":"2024-12-30","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1111/1475-6773.14426","citationCount":"0","resultStr":"{\"title\":\"Associations between rural hospital closures and acute and post-acute care access and outcomes\",\"authors\":\"Geoffrey J. Hoffman PhD, Jinkyung Ha PhD, Zhaohui Fan MD, MPH, Jun Li PhD\",\"doi\":\"10.1111/1475-6773.14426\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<div>\\n \\n \\n <section>\\n \\n <h3> Objective</h3>\\n \\n <p>To determine whether rural hospital closures affected hospital and post-acute care (PAC) use and outcomes.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Study Setting and Design</h3>\\n \\n <p>Using a staggered difference-in-differences design, we evaluated associations between 32 rural hospital closures and changes in county-level: (1) travel distances to and lengths of stay at hospitals; (2) functional limitations at and time from hospital discharge to start of PAC episode; (3) 30-day readmissions and mortality and hospitalizations for a fall-related injury; and (4) population-level hospitalization and death rates.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Data Sources and Analytic Sample</h3>\\n \\n <p>100% Medicare claims and home health and skilled nursing facility clinical data to identify approximately 3 million discharges for older fee-for-service Medicare beneficiaries.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Principal Findings</h3>\\n \\n <p>We found that hospitals that closed compared to those remaining open served more minoritized, lower-income populations, including more Medicaid and fewer commercial patients, and had lower profit margins. Following a closure, quarterly hospitalization rates (111.6 quarterly hospitalizations per 10,000 older adults; 95% CI: 53.4, 170.9) and average hospital lengths of stay increased (0.34 days; 95% CI: 0.13, 0.56 days). We observed no change in the average distance between patients' residential ZIP code and the hospital used (0.29 miles; 95% CI: −1.06, 1.64 miles); average number of standardized ADL limitations at PAC (0.08 SDs from the pre-closure average; 95% CI: −0.12, 0.28 SDs); or PAC time to start (0.02 days; 95% CI: −1.2, 1.2 days). Among more isolated hospitals, closures were associated with an increase in the likelihood of readmission (0.10 percentage-points; 95% CI: 0.00, 0.19).</p>\\n </section>\\n \\n <section>\\n \\n <h3> Conclusions</h3>\\n \\n <p>Closures were not associated with notably worsened health care access, function, or health, potentially because closures triggered care delivery adjustments involving increased numbers of patients seeking out higher quality care.</p>\\n </section>\\n </div>\",\"PeriodicalId\":55065,\"journal\":{\"name\":\"Health Services Research\",\"volume\":\"60 3\",\"pages\":\"\"},\"PeriodicalIF\":3.2000,\"publicationDate\":\"2024-12-30\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://onlinelibrary.wiley.com/doi/epdf/10.1111/1475-6773.14426\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Health Services Research\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://onlinelibrary.wiley.com/doi/10.1111/1475-6773.14426\",\"RegionNum\":2,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"HEALTH CARE SCIENCES & SERVICES\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Health Services Research","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1111/1475-6773.14426","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"HEALTH CARE SCIENCES & SERVICES","Score":null,"Total":0}
Associations between rural hospital closures and acute and post-acute care access and outcomes
Objective
To determine whether rural hospital closures affected hospital and post-acute care (PAC) use and outcomes.
Study Setting and Design
Using a staggered difference-in-differences design, we evaluated associations between 32 rural hospital closures and changes in county-level: (1) travel distances to and lengths of stay at hospitals; (2) functional limitations at and time from hospital discharge to start of PAC episode; (3) 30-day readmissions and mortality and hospitalizations for a fall-related injury; and (4) population-level hospitalization and death rates.
Data Sources and Analytic Sample
100% Medicare claims and home health and skilled nursing facility clinical data to identify approximately 3 million discharges for older fee-for-service Medicare beneficiaries.
Principal Findings
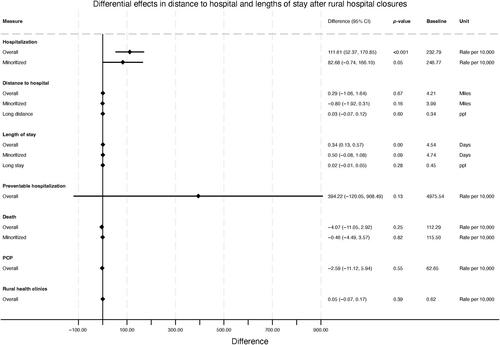
We found that hospitals that closed compared to those remaining open served more minoritized, lower-income populations, including more Medicaid and fewer commercial patients, and had lower profit margins. Following a closure, quarterly hospitalization rates (111.6 quarterly hospitalizations per 10,000 older adults; 95% CI: 53.4, 170.9) and average hospital lengths of stay increased (0.34 days; 95% CI: 0.13, 0.56 days). We observed no change in the average distance between patients' residential ZIP code and the hospital used (0.29 miles; 95% CI: −1.06, 1.64 miles); average number of standardized ADL limitations at PAC (0.08 SDs from the pre-closure average; 95% CI: −0.12, 0.28 SDs); or PAC time to start (0.02 days; 95% CI: −1.2, 1.2 days). Among more isolated hospitals, closures were associated with an increase in the likelihood of readmission (0.10 percentage-points; 95% CI: 0.00, 0.19).
Conclusions
Closures were not associated with notably worsened health care access, function, or health, potentially because closures triggered care delivery adjustments involving increased numbers of patients seeking out higher quality care.
期刊介绍:
Health Services Research (HSR) is a peer-reviewed scholarly journal that provides researchers and public and private policymakers with the latest research findings, methods, and concepts related to the financing, organization, delivery, evaluation, and outcomes of health services. Rated as one of the top journals in the fields of health policy and services and health care administration, HSR publishes outstanding articles reporting the findings of original investigations that expand knowledge and understanding of the wide-ranging field of health care and that will help to improve the health of individuals and communities.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
