Mathilde Stærk, Kasper G Lauridsen, Camilla Thomsen Støtt, Dung Nguyen Riis, Bo Løfgren, Kristian Krogh
{"title":"住院心脏骤停——关键的前5分钟:一项模拟研究","authors":"Mathilde Stærk, Kasper G Lauridsen, Camilla Thomsen Støtt, Dung Nguyen Riis, Bo Løfgren, Kristian Krogh","doi":"10.1186/s41077-022-00225-0","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Early recognition and call for help, fast initiation of chest compressions, and early defibrillation are key elements to improve survival after cardiac arrest but are often not achieved. We aimed to investigate what occurs during the initial treatment of unannounced in situ simulated inhospital cardiac arrests and reasons for successful or inadequate initial resuscitation efforts.</p><p><strong>Methods: </strong>We conducted unannounced full-scale in situ simulated inhospital cardiac arrest followed by a debriefing. Simulations and debriefings were video recorded for subsequent analysis. We analyzed quantitative data on actions performed and time measurements to key actions from simulations and qualitative data from transcribed debriefings.</p><p><strong>Results: </strong>We conducted 36 simulations. Time to diagnosis of cardiac arrest was 37 (27; 55) s. Time to first chest compression from diagnosis of cardiac arrest was 37 (18; 74) s, time to calling the cardiac arrest team was 144 (71; 180) s, and time to first shock was 221 (181; 301) s. We observed participants perform several actions after diagnosing the cardiac arrest and before initiating chest compressions. Domains emerging from the debriefings were teaming and resources. Teaming included the themes communication, role allocation, leadership, and shared knowledge, which all included facilitators and barriers. Resources included the themes knowledge, technical issues, and organizational resources, of which all included barriers, and knowledge also included facilitators.</p><p><strong>Conclusion: </strong>Using unannounced in situ simulated cardiac arrests, we found that key elements such as chest compressions, calling the cardiac arrest team, and defibrillation were delayed. Perceived barriers to resuscitation performance were leadership and teaming, whereas experience, clear leadership, and recent training were perceived as important facilitators for treatment progress.</p>","PeriodicalId":72108,"journal":{"name":"Advances in simulation (London, England)","volume":" ","pages":"29"},"PeriodicalIF":4.7000,"publicationDate":"2022-09-09","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9462625/pdf/","citationCount":"2","resultStr":"{\"title\":\"Inhospital cardiac arrest - the crucial first 5 min: a simulation study.\",\"authors\":\"Mathilde Stærk, Kasper G Lauridsen, Camilla Thomsen Støtt, Dung Nguyen Riis, Bo Løfgren, Kristian Krogh\",\"doi\":\"10.1186/s41077-022-00225-0\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Early recognition and call for help, fast initiation of chest compressions, and early defibrillation are key elements to improve survival after cardiac arrest but are often not achieved. We aimed to investigate what occurs during the initial treatment of unannounced in situ simulated inhospital cardiac arrests and reasons for successful or inadequate initial resuscitation efforts.</p><p><strong>Methods: </strong>We conducted unannounced full-scale in situ simulated inhospital cardiac arrest followed by a debriefing. Simulations and debriefings were video recorded for subsequent analysis. We analyzed quantitative data on actions performed and time measurements to key actions from simulations and qualitative data from transcribed debriefings.</p><p><strong>Results: </strong>We conducted 36 simulations. Time to diagnosis of cardiac arrest was 37 (27; 55) s. Time to first chest compression from diagnosis of cardiac arrest was 37 (18; 74) s, time to calling the cardiac arrest team was 144 (71; 180) s, and time to first shock was 221 (181; 301) s. We observed participants perform several actions after diagnosing the cardiac arrest and before initiating chest compressions. Domains emerging from the debriefings were teaming and resources. Teaming included the themes communication, role allocation, leadership, and shared knowledge, which all included facilitators and barriers. Resources included the themes knowledge, technical issues, and organizational resources, of which all included barriers, and knowledge also included facilitators.</p><p><strong>Conclusion: </strong>Using unannounced in situ simulated cardiac arrests, we found that key elements such as chest compressions, calling the cardiac arrest team, and defibrillation were delayed. Perceived barriers to resuscitation performance were leadership and teaming, whereas experience, clear leadership, and recent training were perceived as important facilitators for treatment progress.</p>\",\"PeriodicalId\":72108,\"journal\":{\"name\":\"Advances in simulation (London, England)\",\"volume\":\" \",\"pages\":\"29\"},\"PeriodicalIF\":4.7000,\"publicationDate\":\"2022-09-09\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9462625/pdf/\",\"citationCount\":\"2\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Advances in simulation (London, England)\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1186/s41077-022-00225-0\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"HEALTH CARE SCIENCES & SERVICES\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Advances in simulation (London, England)","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1186/s41077-022-00225-0","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"HEALTH CARE SCIENCES & SERVICES","Score":null,"Total":0}
Inhospital cardiac arrest - the crucial first 5 min: a simulation study.
Background: Early recognition and call for help, fast initiation of chest compressions, and early defibrillation are key elements to improve survival after cardiac arrest but are often not achieved. We aimed to investigate what occurs during the initial treatment of unannounced in situ simulated inhospital cardiac arrests and reasons for successful or inadequate initial resuscitation efforts.
Methods: We conducted unannounced full-scale in situ simulated inhospital cardiac arrest followed by a debriefing. Simulations and debriefings were video recorded for subsequent analysis. We analyzed quantitative data on actions performed and time measurements to key actions from simulations and qualitative data from transcribed debriefings.
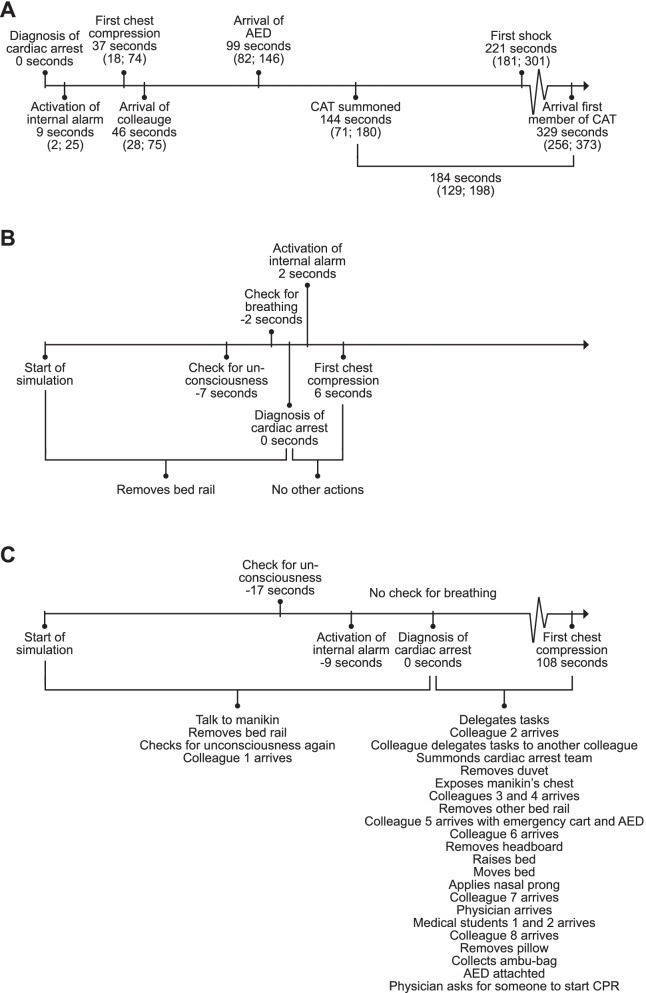
Results: We conducted 36 simulations. Time to diagnosis of cardiac arrest was 37 (27; 55) s. Time to first chest compression from diagnosis of cardiac arrest was 37 (18; 74) s, time to calling the cardiac arrest team was 144 (71; 180) s, and time to first shock was 221 (181; 301) s. We observed participants perform several actions after diagnosing the cardiac arrest and before initiating chest compressions. Domains emerging from the debriefings were teaming and resources. Teaming included the themes communication, role allocation, leadership, and shared knowledge, which all included facilitators and barriers. Resources included the themes knowledge, technical issues, and organizational resources, of which all included barriers, and knowledge also included facilitators.
Conclusion: Using unannounced in situ simulated cardiac arrests, we found that key elements such as chest compressions, calling the cardiac arrest team, and defibrillation were delayed. Perceived barriers to resuscitation performance were leadership and teaming, whereas experience, clear leadership, and recent training were perceived as important facilitators for treatment progress.



 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
