{"title":"关于文章“双心室Takotsubo心肌病与癫痫相关”的回复。","authors":"Ji Yeon Hong","doi":"10.4250/jcu.2016.24.1.88","DOIUrl":null,"url":null,"abstract":"We appreciated the interest of you in our case report.1) Fortunately, we had the previous electrocardiogram (ECG) checked in another hospital 7 years ago, in which there was no Q-waves in leads V1–3 and normal amplitude QRS complexes in limb leads (Fig. 1). Until discharge, we checked the serial ECGs and the ECG of her 2 days of hospitalization started to develop T-wave inversion in leads V5–6 and QT prolongation. The last ECG in our hospital showed persistent low QRS voltages in limb leads and T-wave inversions and QT prolongation in leads V4–6. Also, we found that Q-waves in leads V1–3 lasted despite disappearance of ST segment elevations in V1–3 (Fig. 2). I do not have much clinical experience and have not yet met the patient with recurrent Takotsubo syndrome (TTS) and forme fruste cases of TTS.2) I agree with the idea that the patients with recurrent chest pain and/or dyspnea and normal coronary artery can be diagnosed as TTS. It is not feasible to evaluate the echocardiography as soon as developed chest pain and/or dyspnea, \"smartphone-based technology\" is considered a very useful for diagnosis of unexplained chest pain and/or dyspnea especially in Korea, because Korea is one of the countries with the highest smartphone penetration in the world.3) \n \n \n \nFig. 1 \n \nAn electrocardiogram taken 7 years ago. \n \n \n \n \n \nFig. 2 \n \nAn electrocardiogram obtained before hospital discharge.","PeriodicalId":88913,"journal":{"name":"Journal of cardiovascular ultrasound","volume":"24 1","pages":"88-9"},"PeriodicalIF":0.0000,"publicationDate":"2016-03-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.4250/jcu.2016.24.1.88","citationCount":"0","resultStr":"{\"title\":\"Response to Letter Regarding Article, \\\"Biventricular Takotsubo Cardiomyopathy Associated with Epilepsy\\\".\",\"authors\":\"Ji Yeon Hong\",\"doi\":\"10.4250/jcu.2016.24.1.88\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"We appreciated the interest of you in our case report.1) Fortunately, we had the previous electrocardiogram (ECG) checked in another hospital 7 years ago, in which there was no Q-waves in leads V1–3 and normal amplitude QRS complexes in limb leads (Fig. 1). Until discharge, we checked the serial ECGs and the ECG of her 2 days of hospitalization started to develop T-wave inversion in leads V5–6 and QT prolongation. The last ECG in our hospital showed persistent low QRS voltages in limb leads and T-wave inversions and QT prolongation in leads V4–6. Also, we found that Q-waves in leads V1–3 lasted despite disappearance of ST segment elevations in V1–3 (Fig. 2). I do not have much clinical experience and have not yet met the patient with recurrent Takotsubo syndrome (TTS) and forme fruste cases of TTS.2) I agree with the idea that the patients with recurrent chest pain and/or dyspnea and normal coronary artery can be diagnosed as TTS. It is not feasible to evaluate the echocardiography as soon as developed chest pain and/or dyspnea, \\\"smartphone-based technology\\\" is considered a very useful for diagnosis of unexplained chest pain and/or dyspnea especially in Korea, because Korea is one of the countries with the highest smartphone penetration in the world.3) \\n \\n \\n \\nFig. 1 \\n \\nAn electrocardiogram taken 7 years ago. \\n \\n \\n \\n \\n \\nFig. 2 \\n \\nAn electrocardiogram obtained before hospital discharge.\",\"PeriodicalId\":88913,\"journal\":{\"name\":\"Journal of cardiovascular ultrasound\",\"volume\":\"24 1\",\"pages\":\"88-9\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2016-03-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://sci-hub-pdf.com/10.4250/jcu.2016.24.1.88\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of cardiovascular ultrasound\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.4250/jcu.2016.24.1.88\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2016/3/24 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of cardiovascular ultrasound","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.4250/jcu.2016.24.1.88","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2016/3/24 0:00:00","PubModel":"Epub","JCR":"","JCRName":"","Score":null,"Total":0}
Response to Letter Regarding Article, "Biventricular Takotsubo Cardiomyopathy Associated with Epilepsy".
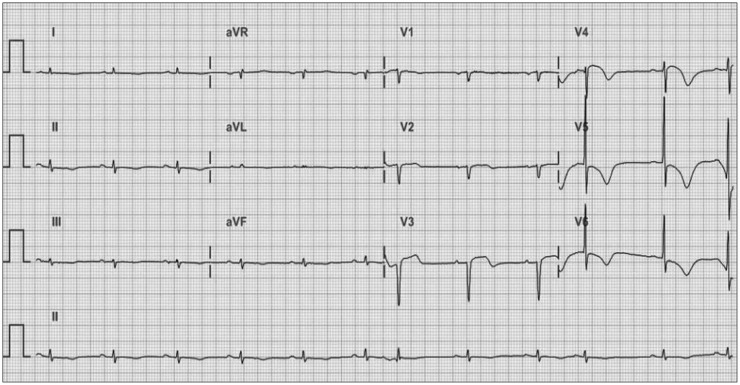
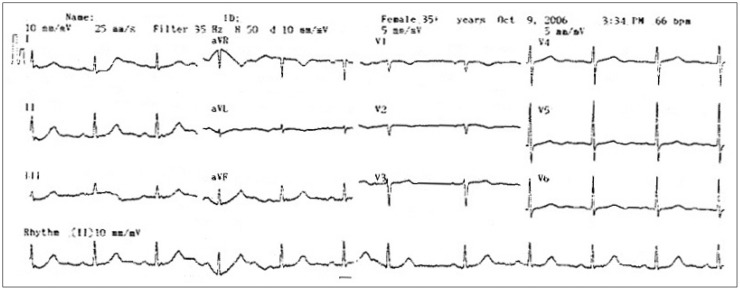
We appreciated the interest of you in our case report.1) Fortunately, we had the previous electrocardiogram (ECG) checked in another hospital 7 years ago, in which there was no Q-waves in leads V1–3 and normal amplitude QRS complexes in limb leads (Fig. 1). Until discharge, we checked the serial ECGs and the ECG of her 2 days of hospitalization started to develop T-wave inversion in leads V5–6 and QT prolongation. The last ECG in our hospital showed persistent low QRS voltages in limb leads and T-wave inversions and QT prolongation in leads V4–6. Also, we found that Q-waves in leads V1–3 lasted despite disappearance of ST segment elevations in V1–3 (Fig. 2). I do not have much clinical experience and have not yet met the patient with recurrent Takotsubo syndrome (TTS) and forme fruste cases of TTS.2) I agree with the idea that the patients with recurrent chest pain and/or dyspnea and normal coronary artery can be diagnosed as TTS. It is not feasible to evaluate the echocardiography as soon as developed chest pain and/or dyspnea, "smartphone-based technology" is considered a very useful for diagnosis of unexplained chest pain and/or dyspnea especially in Korea, because Korea is one of the countries with the highest smartphone penetration in the world.3)
Fig. 1
An electrocardiogram taken 7 years ago.
Fig. 2
An electrocardiogram obtained before hospital discharge.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
