{"title":"定量壁运动分析在急诊科急性胸痛患者中的作用。","authors":"Kyung-Hee Kim, Sang-Hoon Na, Jin-Sik Park","doi":"10.4250/jcu.2017.25.1.20","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Evaluation of acute chest pain in emergency department (ED), using limited resource and time, is still very difficult despite recent development of many diagnostic tools. In this study, we tried to determine the applicability of new semi-automated cardiac function analysis tool, velocity vector imaging (VVI), in the evaluation of the patients with acute chest pain in ED.</p><p><strong>Methods: </strong>We prospectively enrolled 48 patients, who visited ED with acute chest pain, and store images to analyze VVI from July 2005 to July 2007.</p><p><strong>Results: </strong>In 677 of 768 segments (88%), the analysis by VVI was feasible among 48 patients. Peak systolic radial velocity (V<sub>peak</sub>) and strain significantly decreased according to visual regional wall motion abnormality (V<sub>peak</sub>, 3.50 ± 1.34 cm/s for normal vs. 3.46 ± 1.52 cm/s for hypokinesia, 2.51 ± 1.26 for akinesia, <i>p</i> < 0.01; peak systolic radial strain -31.74 ± 9.15% fornormal, -24.33 ± 6.28% for hypokinesia, -20.30 ± 7.78% for akinesia, <i>p</i> < 0.01). However, the velocity vectors at the time of mitral valve opening (MVO) were directed outward in the visually normal myocardium, inward velocity vectors were revealed in the visually akinetic area (V<sub>MVO</sub>, -0.85 ± 1.65 cm/s for normal vs. 0.10 ± 1.46 cm/s for akinesia, <i>p</i> < 0.001). At coronary angiography, V<sub>MVO</sub> clearly increased in the ischemic area (V<sub>MVO</sub>, -0.88+1.56 cm/s for normal vs. 0.70 + 2.04 cm/s for ischemic area, <i>p</i> < 0.01).</p><p><strong>Conclusion: </strong>Regional wall motion assessment using VVI showed could be used to detect significant ischemia in the patient with acute chest pain at ED.</p>","PeriodicalId":88913,"journal":{"name":"Journal of cardiovascular ultrasound","volume":"25 1","pages":"20-27"},"PeriodicalIF":0.0000,"publicationDate":"2017-03-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.4250/jcu.2017.25.1.20","citationCount":"4","resultStr":"{\"title\":\"Role of Quantitative Wall Motion Analysis in Patients with Acute Chest Pain at Emergency Department.\",\"authors\":\"Kyung-Hee Kim, Sang-Hoon Na, Jin-Sik Park\",\"doi\":\"10.4250/jcu.2017.25.1.20\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Evaluation of acute chest pain in emergency department (ED), using limited resource and time, is still very difficult despite recent development of many diagnostic tools. In this study, we tried to determine the applicability of new semi-automated cardiac function analysis tool, velocity vector imaging (VVI), in the evaluation of the patients with acute chest pain in ED.</p><p><strong>Methods: </strong>We prospectively enrolled 48 patients, who visited ED with acute chest pain, and store images to analyze VVI from July 2005 to July 2007.</p><p><strong>Results: </strong>In 677 of 768 segments (88%), the analysis by VVI was feasible among 48 patients. Peak systolic radial velocity (V<sub>peak</sub>) and strain significantly decreased according to visual regional wall motion abnormality (V<sub>peak</sub>, 3.50 ± 1.34 cm/s for normal vs. 3.46 ± 1.52 cm/s for hypokinesia, 2.51 ± 1.26 for akinesia, <i>p</i> < 0.01; peak systolic radial strain -31.74 ± 9.15% fornormal, -24.33 ± 6.28% for hypokinesia, -20.30 ± 7.78% for akinesia, <i>p</i> < 0.01). However, the velocity vectors at the time of mitral valve opening (MVO) were directed outward in the visually normal myocardium, inward velocity vectors were revealed in the visually akinetic area (V<sub>MVO</sub>, -0.85 ± 1.65 cm/s for normal vs. 0.10 ± 1.46 cm/s for akinesia, <i>p</i> < 0.001). At coronary angiography, V<sub>MVO</sub> clearly increased in the ischemic area (V<sub>MVO</sub>, -0.88+1.56 cm/s for normal vs. 0.70 + 2.04 cm/s for ischemic area, <i>p</i> < 0.01).</p><p><strong>Conclusion: </strong>Regional wall motion assessment using VVI showed could be used to detect significant ischemia in the patient with acute chest pain at ED.</p>\",\"PeriodicalId\":88913,\"journal\":{\"name\":\"Journal of cardiovascular ultrasound\",\"volume\":\"25 1\",\"pages\":\"20-27\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2017-03-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://sci-hub-pdf.com/10.4250/jcu.2017.25.1.20\",\"citationCount\":\"4\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of cardiovascular ultrasound\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.4250/jcu.2017.25.1.20\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2017/3/27 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of cardiovascular ultrasound","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.4250/jcu.2017.25.1.20","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2017/3/27 0:00:00","PubModel":"Epub","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 4
摘要
背景:尽管最近发展了许多诊断工具,但急诊部门(ED)急性胸痛的评估仍然非常困难,使用有限的资源和时间。在这项研究中,我们试图确定新的半自动化心功能分析工具——速度矢量成像(VVI)在ED急性胸痛患者评估中的适用性。方法:我们前瞻性地纳入了2005年7月至2007年7月48例因急性胸痛就诊ED的患者,并存储图像以分析VVI。结果:在48例患者中,768个节段中有677个(88%)可用VVI分析。视区壁运动异常显著降低收缩期径向速度峰值(Vpeak)和应变(正常组为3.50±1.34 cm/s,运动不足组为3.46±1.52 cm/s,运动不足组为2.51±1.26 cm/s, p < 0.01;收缩期径向峰值应变正常组为-31.74±9.15%,运动不足组为-24.33±6.28%,运动不足组为-20.30±7.78%,p < 0.01)。然而,在视觉正常的心肌中,二尖瓣打开时的速度矢量向外指向,在视觉运动区显示向内的速度矢量(VMVO,正常心肌为-0.85±1.65 cm/s,运动心肌为0.10±1.46 cm/s, p < 0.001)。冠状动脉造影时,缺血区VMVO明显升高(正常区VMVO为-0.88+1.56 cm/s,缺血区VMVO为0.70 + 2.04 cm/s, p < 0.01)。结论:VVI局部壁运动评价可用于诊断急诊科急性胸痛患者的明显缺血。
Role of Quantitative Wall Motion Analysis in Patients with Acute Chest Pain at Emergency Department.
Background: Evaluation of acute chest pain in emergency department (ED), using limited resource and time, is still very difficult despite recent development of many diagnostic tools. In this study, we tried to determine the applicability of new semi-automated cardiac function analysis tool, velocity vector imaging (VVI), in the evaluation of the patients with acute chest pain in ED.
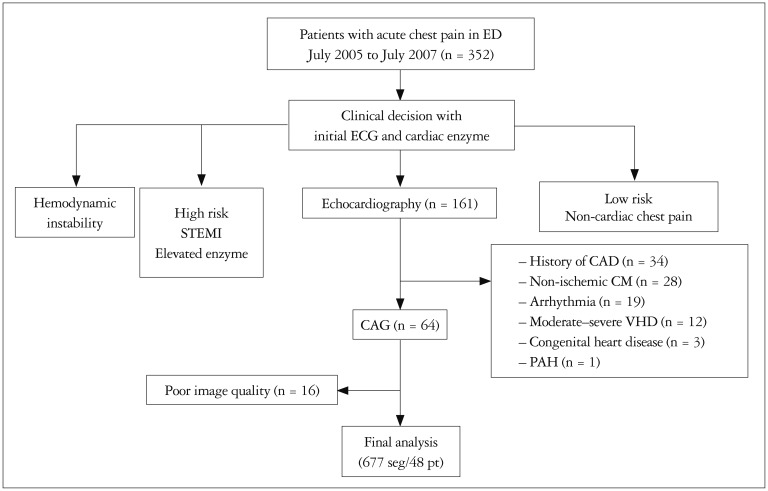
Methods: We prospectively enrolled 48 patients, who visited ED with acute chest pain, and store images to analyze VVI from July 2005 to July 2007.
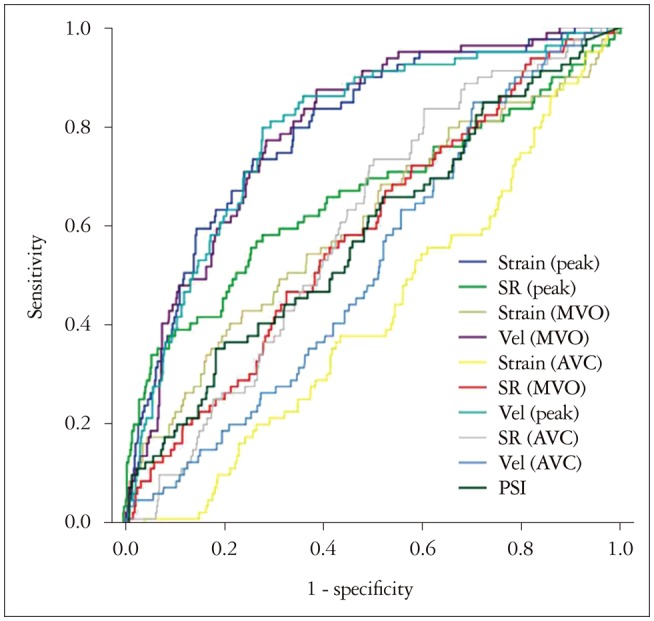
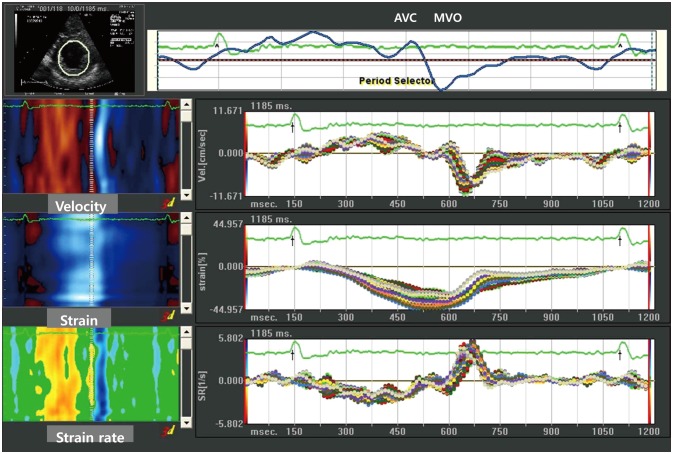
Results: In 677 of 768 segments (88%), the analysis by VVI was feasible among 48 patients. Peak systolic radial velocity (Vpeak) and strain significantly decreased according to visual regional wall motion abnormality (Vpeak, 3.50 ± 1.34 cm/s for normal vs. 3.46 ± 1.52 cm/s for hypokinesia, 2.51 ± 1.26 for akinesia, p < 0.01; peak systolic radial strain -31.74 ± 9.15% fornormal, -24.33 ± 6.28% for hypokinesia, -20.30 ± 7.78% for akinesia, p < 0.01). However, the velocity vectors at the time of mitral valve opening (MVO) were directed outward in the visually normal myocardium, inward velocity vectors were revealed in the visually akinetic area (VMVO, -0.85 ± 1.65 cm/s for normal vs. 0.10 ± 1.46 cm/s for akinesia, p < 0.001). At coronary angiography, VMVO clearly increased in the ischemic area (VMVO, -0.88+1.56 cm/s for normal vs. 0.70 + 2.04 cm/s for ischemic area, p < 0.01).
Conclusion: Regional wall motion assessment using VVI showed could be used to detect significant ischemia in the patient with acute chest pain at ED.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
