{"title":"稳定心脏移植患者的皮质类固醇断奶:血清皮质醇水平的指导。","authors":"David A Baran, Cheryl Rosenfeld, Mark J Zucker","doi":"10.1155/2018/3740395","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Despite earlier studies describing the feasibility of steroid weaning in heart transplant patients, the majority of patients are maintained on steroid therapy for life. We examined a strategy based on a single morning serum cortisol measurement.</p><p><strong>Methods: </strong>We assigned stable posttransplant patients, who were maintained on tacrolimus, mycophenolate mofetil, and corticosteroids, into one of two groups based on a screening morning cortisol level. Patients with a cortisol < 8 micrograms/deciliter were assigned to a \"maintenance\" group and the others were assigned to the weaning group and steroids were tapered off over 4-6 weeks. Patients were monitored on subsequent office visits for adrenal insufficiency and allograft rejection.</p><p><strong>Results: </strong>Thirty-one patients were enrolled (6 patients in the maintenance group and 25 in the steroid-weaning group). Mean follow-up was 10.2 ± 4 years for the weaning group and 9.0 ± 4.9 years in the maintenance group (<i>p</i> = 0.6). No cases of rejection were noted, nor did any patient resume steroid treatment following discontinuation.</p><p><strong>Conclusion: </strong>Steroids can be safely discontinued in stable heart transplant patients with an AM serum cortisol ≥ 8 micrograms/deciliter with appropriate outpatient follow-up. In this study, no patient suffered late rejection or clinically noted adrenal insufficiency.</p>","PeriodicalId":45795,"journal":{"name":"Journal of Transplantation","volume":"2018 ","pages":"3740395"},"PeriodicalIF":2.2000,"publicationDate":"2018-02-18","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.1155/2018/3740395","citationCount":"6","resultStr":"{\"title\":\"Corticosteroid Weaning in Stable Heart Transplant Patients: Guidance by Serum Cortisol Level.\",\"authors\":\"David A Baran, Cheryl Rosenfeld, Mark J Zucker\",\"doi\":\"10.1155/2018/3740395\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Despite earlier studies describing the feasibility of steroid weaning in heart transplant patients, the majority of patients are maintained on steroid therapy for life. We examined a strategy based on a single morning serum cortisol measurement.</p><p><strong>Methods: </strong>We assigned stable posttransplant patients, who were maintained on tacrolimus, mycophenolate mofetil, and corticosteroids, into one of two groups based on a screening morning cortisol level. Patients with a cortisol < 8 micrograms/deciliter were assigned to a \\\"maintenance\\\" group and the others were assigned to the weaning group and steroids were tapered off over 4-6 weeks. Patients were monitored on subsequent office visits for adrenal insufficiency and allograft rejection.</p><p><strong>Results: </strong>Thirty-one patients were enrolled (6 patients in the maintenance group and 25 in the steroid-weaning group). Mean follow-up was 10.2 ± 4 years for the weaning group and 9.0 ± 4.9 years in the maintenance group (<i>p</i> = 0.6). No cases of rejection were noted, nor did any patient resume steroid treatment following discontinuation.</p><p><strong>Conclusion: </strong>Steroids can be safely discontinued in stable heart transplant patients with an AM serum cortisol ≥ 8 micrograms/deciliter with appropriate outpatient follow-up. In this study, no patient suffered late rejection or clinically noted adrenal insufficiency.</p>\",\"PeriodicalId\":45795,\"journal\":{\"name\":\"Journal of Transplantation\",\"volume\":\"2018 \",\"pages\":\"3740395\"},\"PeriodicalIF\":2.2000,\"publicationDate\":\"2018-02-18\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://sci-hub-pdf.com/10.1155/2018/3740395\",\"citationCount\":\"6\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of Transplantation\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1155/2018/3740395\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2018/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q3\",\"JCRName\":\"SURGERY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Transplantation","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1155/2018/3740395","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2018/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"SURGERY","Score":null,"Total":0}
Corticosteroid Weaning in Stable Heart Transplant Patients: Guidance by Serum Cortisol Level.
Background: Despite earlier studies describing the feasibility of steroid weaning in heart transplant patients, the majority of patients are maintained on steroid therapy for life. We examined a strategy based on a single morning serum cortisol measurement.
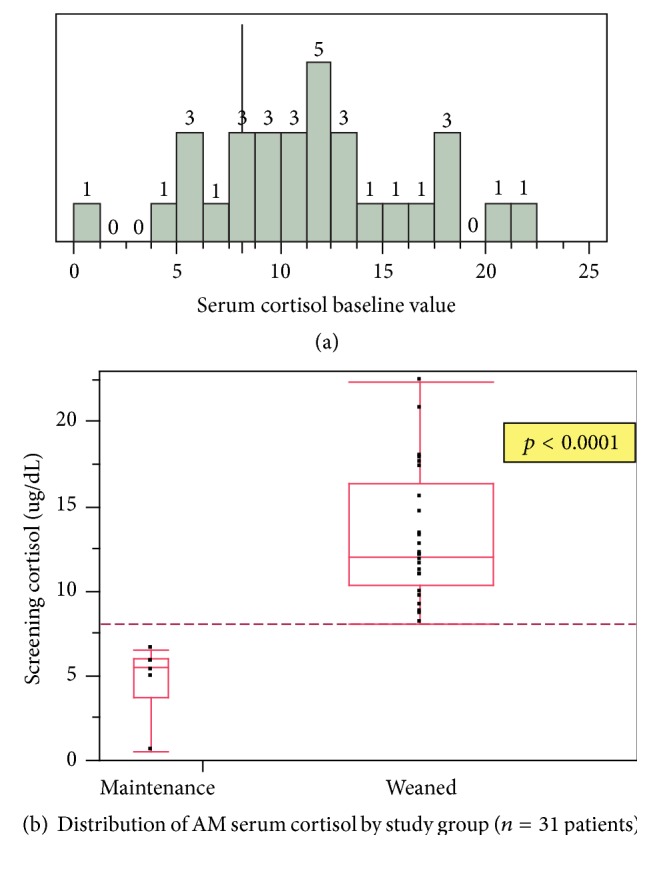
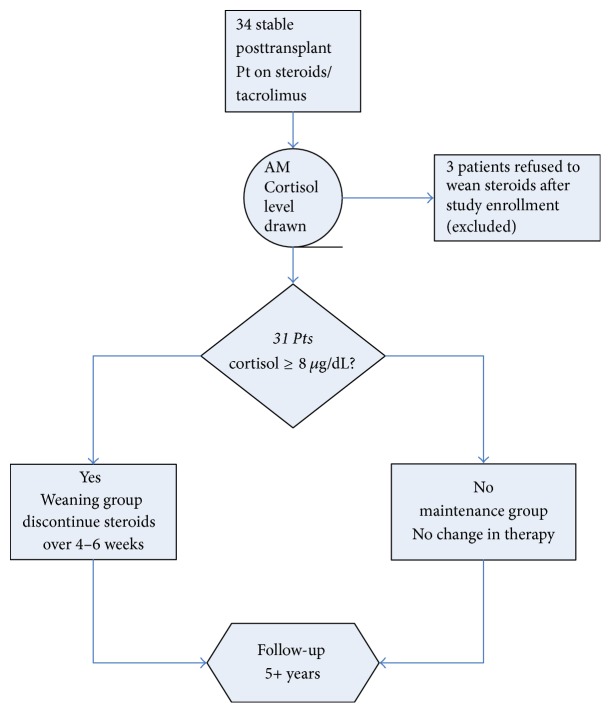
Methods: We assigned stable posttransplant patients, who were maintained on tacrolimus, mycophenolate mofetil, and corticosteroids, into one of two groups based on a screening morning cortisol level. Patients with a cortisol < 8 micrograms/deciliter were assigned to a "maintenance" group and the others were assigned to the weaning group and steroids were tapered off over 4-6 weeks. Patients were monitored on subsequent office visits for adrenal insufficiency and allograft rejection.
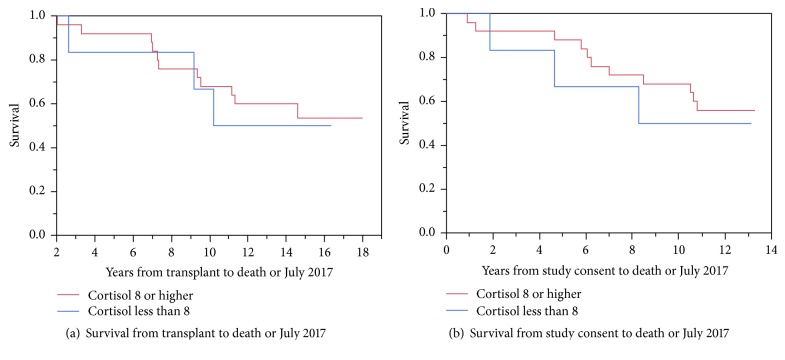
Results: Thirty-one patients were enrolled (6 patients in the maintenance group and 25 in the steroid-weaning group). Mean follow-up was 10.2 ± 4 years for the weaning group and 9.0 ± 4.9 years in the maintenance group (p = 0.6). No cases of rejection were noted, nor did any patient resume steroid treatment following discontinuation.
Conclusion: Steroids can be safely discontinued in stable heart transplant patients with an AM serum cortisol ≥ 8 micrograms/deciliter with appropriate outpatient follow-up. In this study, no patient suffered late rejection or clinically noted adrenal insufficiency.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
