Matthias Waliszewski, Mark Rosenberg, Harald Rittger, Viktor Breul, Florian Krackhardt
{"title":"非劣效性经皮冠状动脉介入试验的终点选择:方法学描述。","authors":"Matthias Waliszewski, Mark Rosenberg, Harald Rittger, Viktor Breul, Florian Krackhardt","doi":"10.1177/1753944720911329","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>The objective of this review is to provide a practical update on endpoint selection for noninferiority (NI) studies in percutaneous coronary intervention studies.</p><p><strong>Methods: </strong>A PubMed search was conducted for predefined terms to explore the use of NI designs and intrapatient comparisons to determine their current importance. Sample size calculations for the most frequently used endpoints with NI hypotheses were done to increase statistical awareness.</p><p><strong>Results: </strong>Reported NI trials, with the most frequently chosen clinical endpoint of major adverse cardiac events (MACE), had NI margins ranging from 1.66% to 5.00%, resulting in patient populations of 400-1500 per treatment group. Clinical study endpoints comprising of MACE complemented with rates of bleeding complications and stent thrombosis (ST) are suggested to conduct a statistically and clinically meaningful NI trial. Study designs with surrogate endpoints amenable to intrapatient randomizations, are a very attractive option to reduce the number of necessary patients by about half. Comparative clinical endpoint studies with MACE and ST/bleeding rates to study a shortened dual antiplatelet therapy (DAPT) in coronary stent trials are feasible, whereas ST as the sole primary endpoint is not useful.</p><p><strong>Conclusions: </strong>Expanded composite clinical endpoints (MACE complemented by ST and bleeding rates and intrapatient randomization for selected surrogate endpoints) may be suitable tools to meet future needs in device approval, recertification and reimbursement.</p>","PeriodicalId":23035,"journal":{"name":"Therapeutic Advances in Cardiovascular Disease","volume":"14 ","pages":"1753944720911329"},"PeriodicalIF":2.6000,"publicationDate":"2020-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.1177/1753944720911329","citationCount":"2","resultStr":"{\"title\":\"Endpoint selection for noninferiority percutaneous coronary intervention trials: a methodological description.\",\"authors\":\"Matthias Waliszewski, Mark Rosenberg, Harald Rittger, Viktor Breul, Florian Krackhardt\",\"doi\":\"10.1177/1753944720911329\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>The objective of this review is to provide a practical update on endpoint selection for noninferiority (NI) studies in percutaneous coronary intervention studies.</p><p><strong>Methods: </strong>A PubMed search was conducted for predefined terms to explore the use of NI designs and intrapatient comparisons to determine their current importance. Sample size calculations for the most frequently used endpoints with NI hypotheses were done to increase statistical awareness.</p><p><strong>Results: </strong>Reported NI trials, with the most frequently chosen clinical endpoint of major adverse cardiac events (MACE), had NI margins ranging from 1.66% to 5.00%, resulting in patient populations of 400-1500 per treatment group. Clinical study endpoints comprising of MACE complemented with rates of bleeding complications and stent thrombosis (ST) are suggested to conduct a statistically and clinically meaningful NI trial. Study designs with surrogate endpoints amenable to intrapatient randomizations, are a very attractive option to reduce the number of necessary patients by about half. Comparative clinical endpoint studies with MACE and ST/bleeding rates to study a shortened dual antiplatelet therapy (DAPT) in coronary stent trials are feasible, whereas ST as the sole primary endpoint is not useful.</p><p><strong>Conclusions: </strong>Expanded composite clinical endpoints (MACE complemented by ST and bleeding rates and intrapatient randomization for selected surrogate endpoints) may be suitable tools to meet future needs in device approval, recertification and reimbursement.</p>\",\"PeriodicalId\":23035,\"journal\":{\"name\":\"Therapeutic Advances in Cardiovascular Disease\",\"volume\":\"14 \",\"pages\":\"1753944720911329\"},\"PeriodicalIF\":2.6000,\"publicationDate\":\"2020-01-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://sci-hub-pdf.com/10.1177/1753944720911329\",\"citationCount\":\"2\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Therapeutic Advances in Cardiovascular Disease\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1177/1753944720911329\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"CARDIAC & CARDIOVASCULAR SYSTEMS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Therapeutic Advances in Cardiovascular Disease","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1177/1753944720911329","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
Endpoint selection for noninferiority percutaneous coronary intervention trials: a methodological description.
Background: The objective of this review is to provide a practical update on endpoint selection for noninferiority (NI) studies in percutaneous coronary intervention studies.
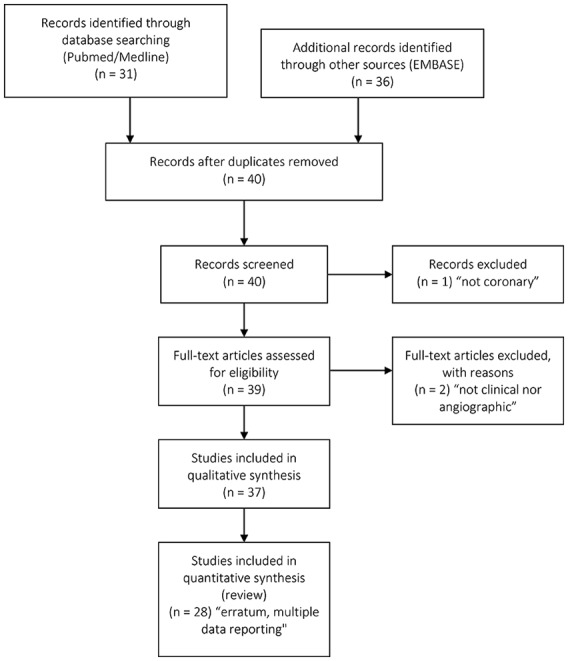
Methods: A PubMed search was conducted for predefined terms to explore the use of NI designs and intrapatient comparisons to determine their current importance. Sample size calculations for the most frequently used endpoints with NI hypotheses were done to increase statistical awareness.
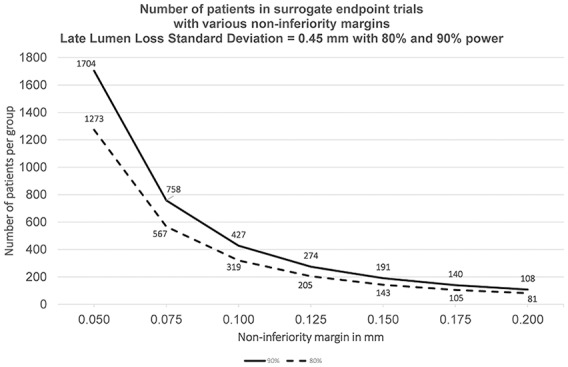
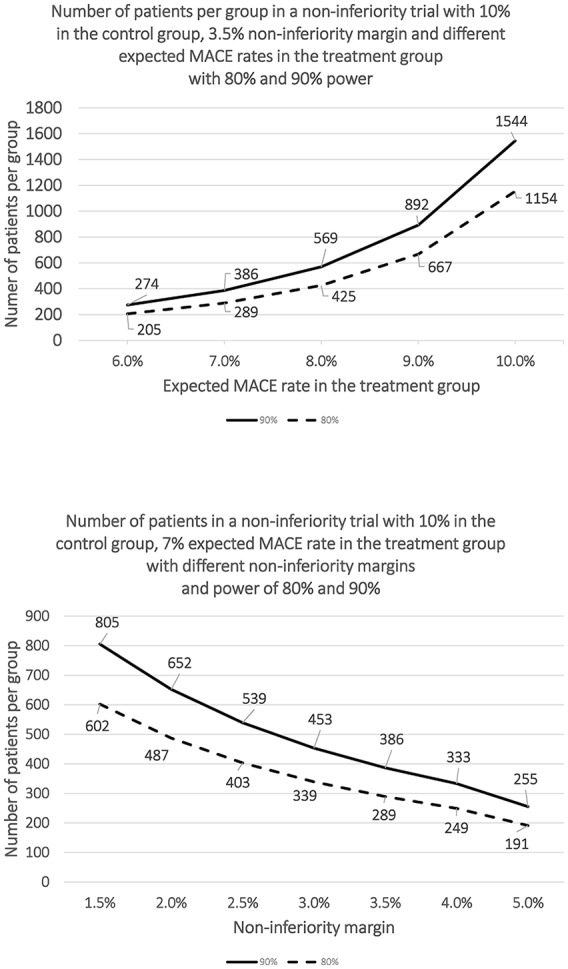
Results: Reported NI trials, with the most frequently chosen clinical endpoint of major adverse cardiac events (MACE), had NI margins ranging from 1.66% to 5.00%, resulting in patient populations of 400-1500 per treatment group. Clinical study endpoints comprising of MACE complemented with rates of bleeding complications and stent thrombosis (ST) are suggested to conduct a statistically and clinically meaningful NI trial. Study designs with surrogate endpoints amenable to intrapatient randomizations, are a very attractive option to reduce the number of necessary patients by about half. Comparative clinical endpoint studies with MACE and ST/bleeding rates to study a shortened dual antiplatelet therapy (DAPT) in coronary stent trials are feasible, whereas ST as the sole primary endpoint is not useful.
Conclusions: Expanded composite clinical endpoints (MACE complemented by ST and bleeding rates and intrapatient randomization for selected surrogate endpoints) may be suitable tools to meet future needs in device approval, recertification and reimbursement.
期刊介绍:
The journal is aimed at clinicians and researchers from the cardiovascular disease field and will be a forum for all views and reviews relating to this discipline.Topics covered will include: ·arteriosclerosis ·cardiomyopathies ·coronary artery disease ·diabetes ·heart failure ·hypertension ·metabolic syndrome ·obesity ·peripheral arterial disease ·stroke ·arrhythmias ·genetics



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
