Claire W. Rothschild , Barbra A. Richardson , Brandon L. Guthrie , Peninah Kithao , Tom Omurwa , James Mukabi , Erica M Lokken , Grace John-Stewart , Jennifer A. Unger , John Kinuthia , Alison L. Drake
{"title":"一个风险评分工具,用于预测肯尼亚妇女在避孕中止的高风险","authors":"Claire W. Rothschild , Barbra A. Richardson , Brandon L. Guthrie , Peninah Kithao , Tom Omurwa , James Mukabi , Erica M Lokken , Grace John-Stewart , Jennifer A. Unger , John Kinuthia , Alison L. Drake","doi":"10.1016/j.conx.2020.100045","DOIUrl":null,"url":null,"abstract":"<div><h3>Objective</h3><p>We developed and validated a pragmatic risk assessment tool for identifying contraceptive discontinuation among Kenyan women who do not desire pregnancy.</p></div><div><h3>Study design</h3><p>Within a prospective cohort of contraceptive users, participants were randomly allocated to derivation (<em>n</em> = 558) and validation (<em>n</em> = 186) cohorts. Risk scores were developed by selecting the Cox proportional hazards model with the minimum Akaike information criterion. Predictive performance was evaluated using time-dependent receiver operating characteristic curves and area under the curve (AUC).</p></div><div><h3>Results</h3><p>The overall contraceptive discontinuation rate was 36.9 per 100 woman-years (95% confidence interval [CI] 30.3–44.9). The predictors of discontinuation selected for the risk score included use of a short-term method or copper intrauterine device (vs. injectable or implant), method continuation or switch (vs. initiation), <<!--> <!-->9 years of completed education, not having a child aged <<!--> <!-->6 months, and having no spouse or a spouse supportive of family planning (vs. having a spouse who has unsupportive or uncertain attitudes towards family planning). AUC at 24 weeks was 0.76 (95% CI 0.64–0.87) with 70.0% sensitivity and 78.6% specificity at the optimal cut point in the derivation cohort. Discontinuation was 3.8-fold higher among high- vs. low-risk women (95% CI 2.33–6.30). AUC was 0.68 (95% CI 0.47–0.90) in the validation cohort. A simplified score comprising routinely collected variables demonstrated similar performance (derivation-AUC: 0.73 [95% CI 0.60–0.85]; validation-AUC: 0.73 [95% CI 0.51–0.94]). Positive predictive value in the derivation cohort was 31.4% for the full and 28.1% for the simplified score.</p></div><div><h3>Conclusions</h3><p>The risk scores demonstrated moderate predictive ability but identified large proportions of women as high risk. Future research is needed to improve sensitivity and specificity of a clinical tool to identify women at high risk for experiencing method-related challenges.</p></div><div><h3>Implications</h3><p>Contraceptive discontinuation is a major driver of unmet contraceptive need globally. Few tools exist for identifying women who may benefit most from additional support in order to meet their contraceptive needs and preferences. This study developed and assessed the validity of a provider-focused risk prediction tool for contraceptive discontinuation among Kenyan women using modern contraception. High rates of early discontinuation observed in this study emphasize the necessity of investing in efforts to develop new contraceptive technologies and stronger delivery systems to better align with women's needs and preferences for voluntary family planning.</p></div>","PeriodicalId":10655,"journal":{"name":"Contraception: X","volume":"2 ","pages":"Article 100045"},"PeriodicalIF":0.0000,"publicationDate":"2020-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.1016/j.conx.2020.100045","citationCount":"1","resultStr":"{\"title\":\"A risk scoring tool for predicting Kenyan women at high risk of contraceptive discontinuation\",\"authors\":\"Claire W. Rothschild , Barbra A. Richardson , Brandon L. Guthrie , Peninah Kithao , Tom Omurwa , James Mukabi , Erica M Lokken , Grace John-Stewart , Jennifer A. Unger , John Kinuthia , Alison L. Drake\",\"doi\":\"10.1016/j.conx.2020.100045\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<div><h3>Objective</h3><p>We developed and validated a pragmatic risk assessment tool for identifying contraceptive discontinuation among Kenyan women who do not desire pregnancy.</p></div><div><h3>Study design</h3><p>Within a prospective cohort of contraceptive users, participants were randomly allocated to derivation (<em>n</em> = 558) and validation (<em>n</em> = 186) cohorts. Risk scores were developed by selecting the Cox proportional hazards model with the minimum Akaike information criterion. Predictive performance was evaluated using time-dependent receiver operating characteristic curves and area under the curve (AUC).</p></div><div><h3>Results</h3><p>The overall contraceptive discontinuation rate was 36.9 per 100 woman-years (95% confidence interval [CI] 30.3–44.9). The predictors of discontinuation selected for the risk score included use of a short-term method or copper intrauterine device (vs. injectable or implant), method continuation or switch (vs. initiation), <<!--> <!-->9 years of completed education, not having a child aged <<!--> <!-->6 months, and having no spouse or a spouse supportive of family planning (vs. having a spouse who has unsupportive or uncertain attitudes towards family planning). AUC at 24 weeks was 0.76 (95% CI 0.64–0.87) with 70.0% sensitivity and 78.6% specificity at the optimal cut point in the derivation cohort. Discontinuation was 3.8-fold higher among high- vs. low-risk women (95% CI 2.33–6.30). AUC was 0.68 (95% CI 0.47–0.90) in the validation cohort. A simplified score comprising routinely collected variables demonstrated similar performance (derivation-AUC: 0.73 [95% CI 0.60–0.85]; validation-AUC: 0.73 [95% CI 0.51–0.94]). Positive predictive value in the derivation cohort was 31.4% for the full and 28.1% for the simplified score.</p></div><div><h3>Conclusions</h3><p>The risk scores demonstrated moderate predictive ability but identified large proportions of women as high risk. Future research is needed to improve sensitivity and specificity of a clinical tool to identify women at high risk for experiencing method-related challenges.</p></div><div><h3>Implications</h3><p>Contraceptive discontinuation is a major driver of unmet contraceptive need globally. Few tools exist for identifying women who may benefit most from additional support in order to meet their contraceptive needs and preferences. This study developed and assessed the validity of a provider-focused risk prediction tool for contraceptive discontinuation among Kenyan women using modern contraception. High rates of early discontinuation observed in this study emphasize the necessity of investing in efforts to develop new contraceptive technologies and stronger delivery systems to better align with women's needs and preferences for voluntary family planning.</p></div>\",\"PeriodicalId\":10655,\"journal\":{\"name\":\"Contraception: X\",\"volume\":\"2 \",\"pages\":\"Article 100045\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2020-01-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://sci-hub-pdf.com/10.1016/j.conx.2020.100045\",\"citationCount\":\"1\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Contraception: X\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://www.sciencedirect.com/science/article/pii/S2590151620300289\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2020/10/29 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q2\",\"JCRName\":\"Medicine\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Contraception: X","FirstCategoryId":"1085","ListUrlMain":"https://www.sciencedirect.com/science/article/pii/S2590151620300289","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2020/10/29 0:00:00","PubModel":"Epub","JCR":"Q2","JCRName":"Medicine","Score":null,"Total":0}
引用次数: 1
摘要
目的:我们开发并验证了一种实用的风险评估工具,用于在不希望怀孕的肯尼亚妇女中识别避孕药停药。研究设计:在前瞻性避孕药使用者队列中,参与者被随机分配到衍生队列(n = 558)和验证队列(n = 186)。采用最小赤池信息准则的Cox比例风险模型进行风险评分。使用随时间变化的受试者工作特征曲线和曲线下面积(AUC)评估预测性能。结果总体避孕药停药率为36.9 / 100名妇女年(95%可信区间[CI] 30.3 ~ 44.9)。选择用于风险评分的停药预测因素包括使用短期方法或铜质宫内节育器(相对于注射或植入),方法继续或转换(相对于起始),<9 已完成教育年数,无子女;6 个月,没有配偶或配偶支持计划生育(配偶对计划生育不支持或态度不确定)。在衍生队列中,24 周时的AUC为0.76 (95% CI 0.64-0.87),敏感性为70.0%,特异性为78.6%。高危妇女的停药率是低危妇女的3.8倍(95% CI 2.33-6.30)。验证队列的AUC为0.68 (95% CI 0.47-0.90)。由常规收集的变量组成的简化评分显示出类似的表现(导数auc: 0.73 [95% CI 0.60-0.85];验证- auc: 0.73 [95% CI 0.51-0.94])。在衍生队列中,完整评分的阳性预测值为31.4%,简化评分为28.1%。结论风险评分显示出中等的预测能力,但确定了很大比例的女性为高风险。未来的研究需要提高临床工具的敏感性和特异性,以识别经历方法相关挑战的高风险妇女。终止避孕是全球避孕需求未得到满足的主要驱动因素。现有的工具很少,无法确定哪些妇女可能从满足其避孕需要和偏好的额外支助中获益最多。本研究开发并评估了一种以提供者为中心的风险预测工具的有效性,该工具适用于使用现代避孕方法的肯尼亚妇女。本研究中观察到的早期中止率很高,强调必须投资开发新的避孕技术和更强有力的提供系统,以便更好地符合妇女自愿计划生育的需要和偏好。
A risk scoring tool for predicting Kenyan women at high risk of contraceptive discontinuation
Objective
We developed and validated a pragmatic risk assessment tool for identifying contraceptive discontinuation among Kenyan women who do not desire pregnancy.
Study design
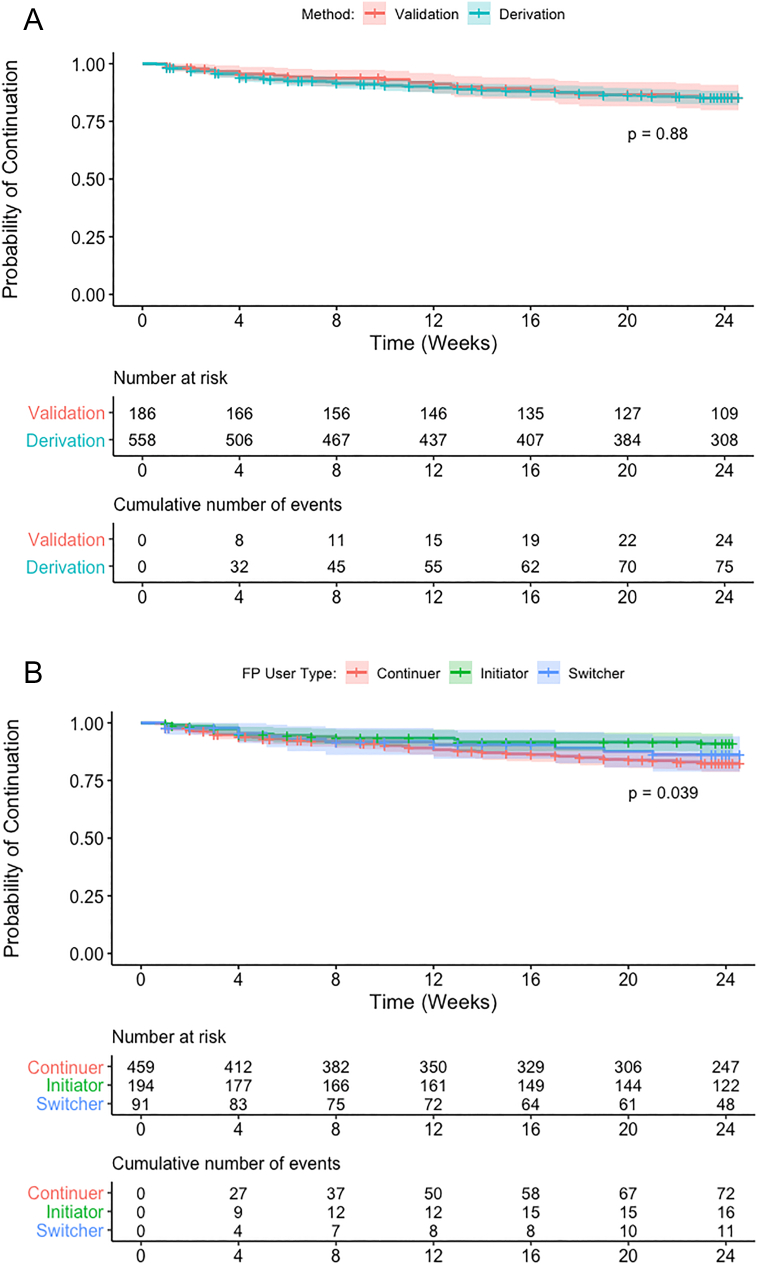
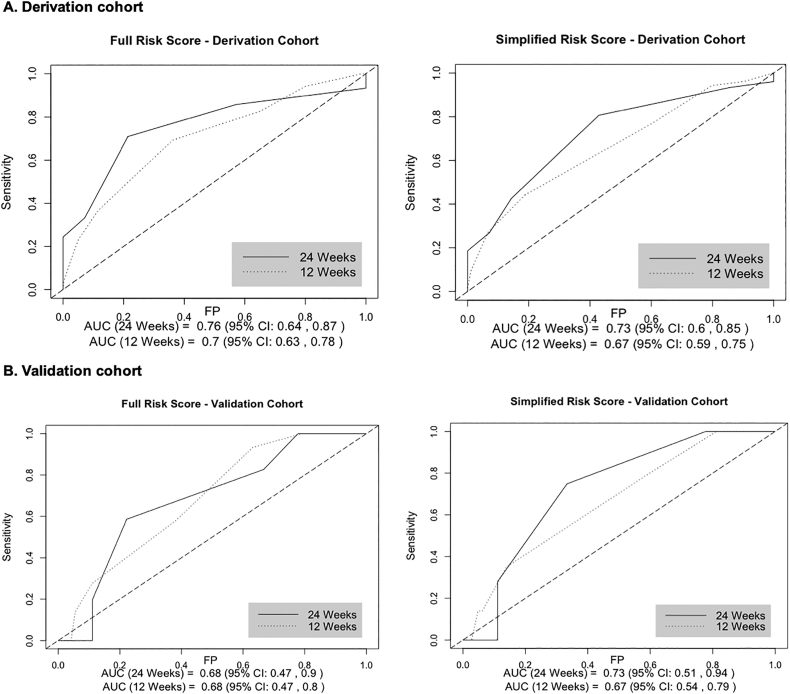
Within a prospective cohort of contraceptive users, participants were randomly allocated to derivation (n = 558) and validation (n = 186) cohorts. Risk scores were developed by selecting the Cox proportional hazards model with the minimum Akaike information criterion. Predictive performance was evaluated using time-dependent receiver operating characteristic curves and area under the curve (AUC).
Results
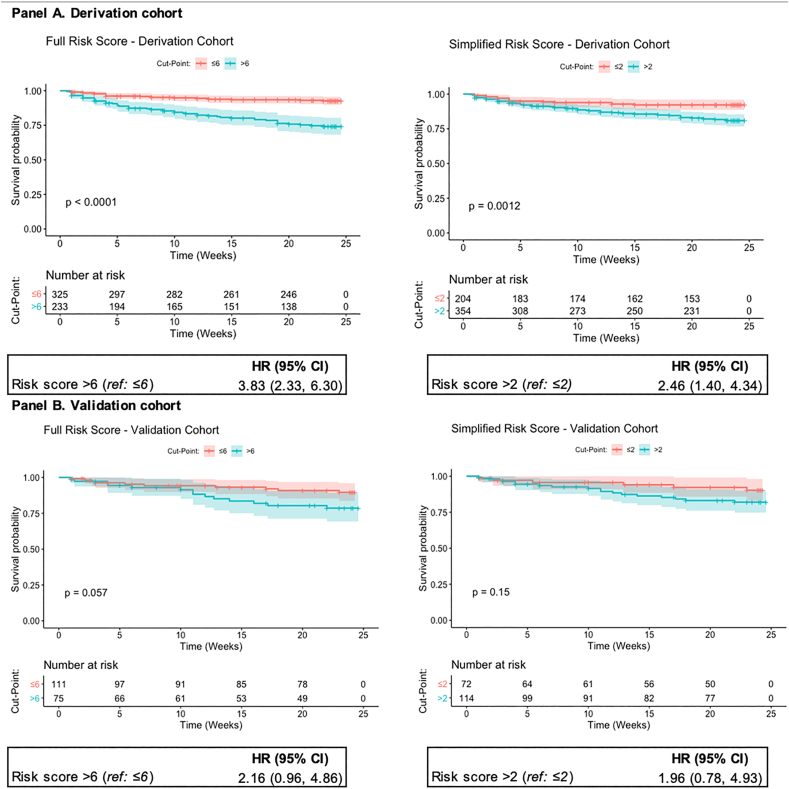
The overall contraceptive discontinuation rate was 36.9 per 100 woman-years (95% confidence interval [CI] 30.3–44.9). The predictors of discontinuation selected for the risk score included use of a short-term method or copper intrauterine device (vs. injectable or implant), method continuation or switch (vs. initiation), < 9 years of completed education, not having a child aged < 6 months, and having no spouse or a spouse supportive of family planning (vs. having a spouse who has unsupportive or uncertain attitudes towards family planning). AUC at 24 weeks was 0.76 (95% CI 0.64–0.87) with 70.0% sensitivity and 78.6% specificity at the optimal cut point in the derivation cohort. Discontinuation was 3.8-fold higher among high- vs. low-risk women (95% CI 2.33–6.30). AUC was 0.68 (95% CI 0.47–0.90) in the validation cohort. A simplified score comprising routinely collected variables demonstrated similar performance (derivation-AUC: 0.73 [95% CI 0.60–0.85]; validation-AUC: 0.73 [95% CI 0.51–0.94]). Positive predictive value in the derivation cohort was 31.4% for the full and 28.1% for the simplified score.
Conclusions
The risk scores demonstrated moderate predictive ability but identified large proportions of women as high risk. Future research is needed to improve sensitivity and specificity of a clinical tool to identify women at high risk for experiencing method-related challenges.
Implications
Contraceptive discontinuation is a major driver of unmet contraceptive need globally. Few tools exist for identifying women who may benefit most from additional support in order to meet their contraceptive needs and preferences. This study developed and assessed the validity of a provider-focused risk prediction tool for contraceptive discontinuation among Kenyan women using modern contraception. High rates of early discontinuation observed in this study emphasize the necessity of investing in efforts to develop new contraceptive technologies and stronger delivery systems to better align with women's needs and preferences for voluntary family planning.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
