Krishnaraj Sinhji Rathod, Marco Spagnolo, Mark K Elliott, Anne-Marie Beirne, Elliot J Smith, Rajiv Amersey, Charles Knight, Roshan Weerackody, Andreas Baumbach, Anthony Mathur, Daniel A Jones
{"title":"一项观察性研究评估多血管疾病患者接受原发性经皮冠状动脉介入治疗的立即完全与延迟完全血运重建。","authors":"Krishnaraj Sinhji Rathod, Marco Spagnolo, Mark K Elliott, Anne-Marie Beirne, Elliot J Smith, Rajiv Amersey, Charles Knight, Roshan Weerackody, Andreas Baumbach, Anthony Mathur, Daniel A Jones","doi":"10.1177/1179546820951792","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>More than half of the patients undergoing primary percutaneous coronary intervention (PCI) for ST-segment elevation myocardial infarction (STEMI) have multi-vessel coronary artery disease. This is associated with worse outcomes compared with single vessel disease. Whilst evidence now exists to support complete revascularisation for bystander disease the optimal timing is still debated. This study aimed to compare clinical outcomes in patients with STEMI and multi-vessel disease who underwent complete revascularisation as inpatients in comparison to patients who had staged PCI as early outpatients.</p><p><strong>Methods and results: </strong>We conducted an observational cohort study consisting of 1522 patients who underwent primary PCI with multi-vessel disease from 2012 to 2019. Exclusions included patients with cardiogenic shock and previous CABG. Patients were split into 2 groups depending on whether they had complete revascularisation performed as inpatients or as staged PCI at later outpatient dates. The primary outcome of this study was major adverse cardiac events (consisting of myocardial infarction, target vessel revascularisation and all-cause mortality).834 (54.8%) patients underwent complete inpatient revascularisation and 688 patients (45.2%) had outpatient PCI (median 43 days post discharge). Of the inpatient group, 652 patients (78.2%) underwent complete revascularisation during the index procedure whilst 182 (21.8%) patients underwent inpatient bystander PCI in a second procedure. Overall, there were no significant differences between the groups with regards to their baseline or procedural characteristics. Over the follow-up period there was no significant difference in MACE between the cohorts (<i>P</i> = .62), which persisted after multivariate adjustment (HR 1.21 [95% CI 0.72-1.96]). Furthermore, in propensity-matched analysis there was no significant difference in outcome between the groups (HR: 0.86 95% CI: 0.75-1.25).</p><p><strong>Conclusions: </strong>Our study demonstrated that the timing of bystander PCI after STEMI did not appear to have an effect on cardiovascular outcomes. We suggest that patients with multi-vessel disease can potentially be discharged promptly and undergo early outpatient bystander PCI. This could significantly reduce length of stay in hospital.</p>","PeriodicalId":10419,"journal":{"name":"Clinical Medicine Insights. Cardiology","volume":"14 ","pages":"1179546820951792"},"PeriodicalIF":3.3000,"publicationDate":"2020-08-21","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/46/fd/10.1177_1179546820951792.PMC7444144.pdf","citationCount":"0","resultStr":"{\"title\":\"An Observational Study Assessing Immediate Complete Versus Delayed Complete Revascularisation in Patients with Multi-Vessel Disease Undergoing Primary Percutaneous Coronary Intervention.\",\"authors\":\"Krishnaraj Sinhji Rathod, Marco Spagnolo, Mark K Elliott, Anne-Marie Beirne, Elliot J Smith, Rajiv Amersey, Charles Knight, Roshan Weerackody, Andreas Baumbach, Anthony Mathur, Daniel A Jones\",\"doi\":\"10.1177/1179546820951792\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>More than half of the patients undergoing primary percutaneous coronary intervention (PCI) for ST-segment elevation myocardial infarction (STEMI) have multi-vessel coronary artery disease. This is associated with worse outcomes compared with single vessel disease. Whilst evidence now exists to support complete revascularisation for bystander disease the optimal timing is still debated. This study aimed to compare clinical outcomes in patients with STEMI and multi-vessel disease who underwent complete revascularisation as inpatients in comparison to patients who had staged PCI as early outpatients.</p><p><strong>Methods and results: </strong>We conducted an observational cohort study consisting of 1522 patients who underwent primary PCI with multi-vessel disease from 2012 to 2019. Exclusions included patients with cardiogenic shock and previous CABG. Patients were split into 2 groups depending on whether they had complete revascularisation performed as inpatients or as staged PCI at later outpatient dates. The primary outcome of this study was major adverse cardiac events (consisting of myocardial infarction, target vessel revascularisation and all-cause mortality).834 (54.8%) patients underwent complete inpatient revascularisation and 688 patients (45.2%) had outpatient PCI (median 43 days post discharge). Of the inpatient group, 652 patients (78.2%) underwent complete revascularisation during the index procedure whilst 182 (21.8%) patients underwent inpatient bystander PCI in a second procedure. Overall, there were no significant differences between the groups with regards to their baseline or procedural characteristics. Over the follow-up period there was no significant difference in MACE between the cohorts (<i>P</i> = .62), which persisted after multivariate adjustment (HR 1.21 [95% CI 0.72-1.96]). Furthermore, in propensity-matched analysis there was no significant difference in outcome between the groups (HR: 0.86 95% CI: 0.75-1.25).</p><p><strong>Conclusions: </strong>Our study demonstrated that the timing of bystander PCI after STEMI did not appear to have an effect on cardiovascular outcomes. We suggest that patients with multi-vessel disease can potentially be discharged promptly and undergo early outpatient bystander PCI. This could significantly reduce length of stay in hospital.</p>\",\"PeriodicalId\":10419,\"journal\":{\"name\":\"Clinical Medicine Insights. Cardiology\",\"volume\":\"14 \",\"pages\":\"1179546820951792\"},\"PeriodicalIF\":3.3000,\"publicationDate\":\"2020-08-21\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/46/fd/10.1177_1179546820951792.PMC7444144.pdf\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Clinical Medicine Insights. Cardiology\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1177/1179546820951792\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2020/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q2\",\"JCRName\":\"CARDIAC & CARDIOVASCULAR SYSTEMS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Clinical Medicine Insights. Cardiology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1177/1179546820951792","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2020/1/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
An Observational Study Assessing Immediate Complete Versus Delayed Complete Revascularisation in Patients with Multi-Vessel Disease Undergoing Primary Percutaneous Coronary Intervention.
Background: More than half of the patients undergoing primary percutaneous coronary intervention (PCI) for ST-segment elevation myocardial infarction (STEMI) have multi-vessel coronary artery disease. This is associated with worse outcomes compared with single vessel disease. Whilst evidence now exists to support complete revascularisation for bystander disease the optimal timing is still debated. This study aimed to compare clinical outcomes in patients with STEMI and multi-vessel disease who underwent complete revascularisation as inpatients in comparison to patients who had staged PCI as early outpatients.
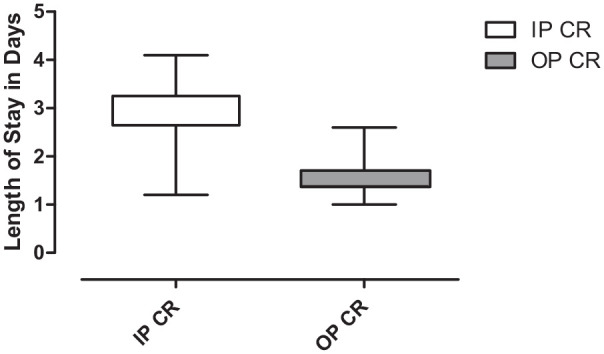
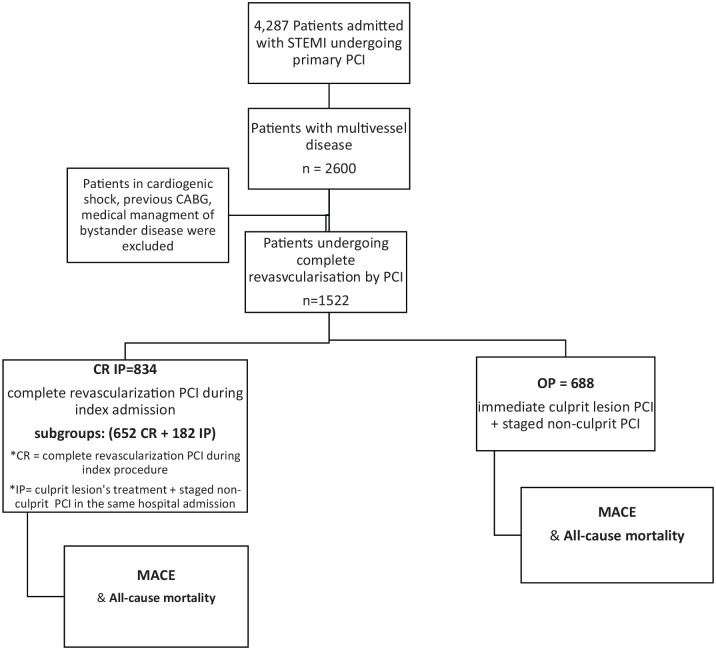
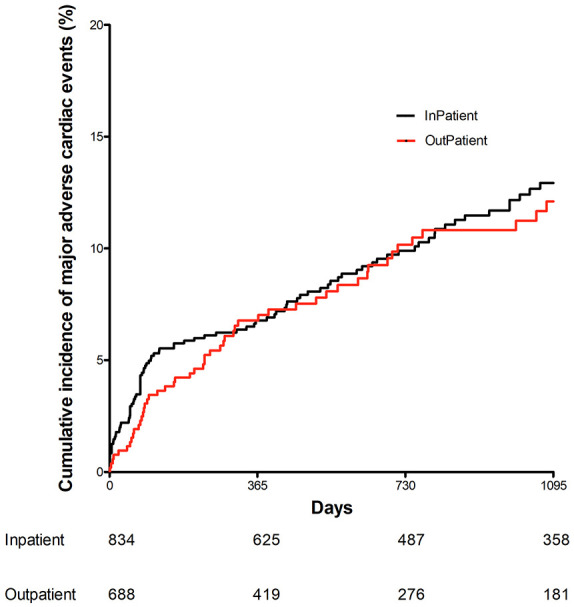
Methods and results: We conducted an observational cohort study consisting of 1522 patients who underwent primary PCI with multi-vessel disease from 2012 to 2019. Exclusions included patients with cardiogenic shock and previous CABG. Patients were split into 2 groups depending on whether they had complete revascularisation performed as inpatients or as staged PCI at later outpatient dates. The primary outcome of this study was major adverse cardiac events (consisting of myocardial infarction, target vessel revascularisation and all-cause mortality).834 (54.8%) patients underwent complete inpatient revascularisation and 688 patients (45.2%) had outpatient PCI (median 43 days post discharge). Of the inpatient group, 652 patients (78.2%) underwent complete revascularisation during the index procedure whilst 182 (21.8%) patients underwent inpatient bystander PCI in a second procedure. Overall, there were no significant differences between the groups with regards to their baseline or procedural characteristics. Over the follow-up period there was no significant difference in MACE between the cohorts (P = .62), which persisted after multivariate adjustment (HR 1.21 [95% CI 0.72-1.96]). Furthermore, in propensity-matched analysis there was no significant difference in outcome between the groups (HR: 0.86 95% CI: 0.75-1.25).
Conclusions: Our study demonstrated that the timing of bystander PCI after STEMI did not appear to have an effect on cardiovascular outcomes. We suggest that patients with multi-vessel disease can potentially be discharged promptly and undergo early outpatient bystander PCI. This could significantly reduce length of stay in hospital.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
