Swathi Subramany, Ajoe John Kattoor, Swathi Kovelamudi, Subodh Devabhaktuni, Jawahar L Mehta, Srikanth Vallurupalli, Hakan Paydak, Naga Venkata K Pothineni
{"title":"下导联q波在室性心动过速诊断中的应用。","authors":"Swathi Subramany, Ajoe John Kattoor, Swathi Kovelamudi, Subodh Devabhaktuni, Jawahar L Mehta, Srikanth Vallurupalli, Hakan Paydak, Naga Venkata K Pothineni","doi":"10.1177/1179546820953416","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Electrocardiogram (ECG) differentiation of wide complex tachycardia (WCT) into ventricular tachycardia (VT) and supraventricular tachycardia with aberration (SVT-A) is often challenging.</p><p><strong>Objective: </strong>To determine if the presence of Q-waveforms (QS, Qr, QRs) in the inferior leads (II, III, aVF) can differentiate VT from SVT-A in a WCT compared to Brugada algorithm. We studied 2 inferior lead criteria namely QWC-A where all the inferior leads had a similar Q wave pattern and QWC-B where only lead aVF had a Q-waveform.</p><p><strong>Methods: </strong>A total of 181 consecutive cases of WCT were identified, digitally separated into precordial leads and inferior leads and independently reviewed by 2 electrophysiologists. An electrocardiographic diagnosis of VT or SVT-A was assigned based on Brugada and inferior lead algorithms. Results were compared to the final clinical diagnosis.</p><p><strong>Results: </strong>VT was the final clinical diagnosis in 24.9% of ECG cohort (45/181); 75.1% (136/181) were SVT-A. QWC-A and QWC-B had a high specificity (93.3% and 82.8%) and accuracy (78.2% and 71.0%), but low sensitivity (33.3% and 35.6%) in differentiating VT from SVT-A. The Brugada algorithm yielded a sensitivity of 82.2% and specificity of 68.4%. Area under the curve in ROC analysis was highest with Brugada algorithm (0.75, 95% CI 0.69-0.81) followed by QWC-A (0.63, 95% CI 0.56-0.70) and QWC-B (0.59, 95% CI 0.52-0.67).</p><p><strong>Conclusion: </strong>QWC-A and QWC-B criteria had poor sensitivity but high specificity in diagnosing VT in patients presenting with WCT. Further research combining this simple criterion with other newer diagnostic algorithms can potentially improve the accuracy of the overall diagnostic algorithm.</p>","PeriodicalId":10419,"journal":{"name":"Clinical Medicine Insights. Cardiology","volume":"14 ","pages":"1179546820953416"},"PeriodicalIF":3.3000,"publicationDate":"2020-08-30","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.1177/1179546820953416","citationCount":"2","resultStr":"{\"title\":\"Utility of Inferior Lead Q-waveforms in diagnosing Ventricular Tachycardia.\",\"authors\":\"Swathi Subramany, Ajoe John Kattoor, Swathi Kovelamudi, Subodh Devabhaktuni, Jawahar L Mehta, Srikanth Vallurupalli, Hakan Paydak, Naga Venkata K Pothineni\",\"doi\":\"10.1177/1179546820953416\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Electrocardiogram (ECG) differentiation of wide complex tachycardia (WCT) into ventricular tachycardia (VT) and supraventricular tachycardia with aberration (SVT-A) is often challenging.</p><p><strong>Objective: </strong>To determine if the presence of Q-waveforms (QS, Qr, QRs) in the inferior leads (II, III, aVF) can differentiate VT from SVT-A in a WCT compared to Brugada algorithm. We studied 2 inferior lead criteria namely QWC-A where all the inferior leads had a similar Q wave pattern and QWC-B where only lead aVF had a Q-waveform.</p><p><strong>Methods: </strong>A total of 181 consecutive cases of WCT were identified, digitally separated into precordial leads and inferior leads and independently reviewed by 2 electrophysiologists. An electrocardiographic diagnosis of VT or SVT-A was assigned based on Brugada and inferior lead algorithms. Results were compared to the final clinical diagnosis.</p><p><strong>Results: </strong>VT was the final clinical diagnosis in 24.9% of ECG cohort (45/181); 75.1% (136/181) were SVT-A. QWC-A and QWC-B had a high specificity (93.3% and 82.8%) and accuracy (78.2% and 71.0%), but low sensitivity (33.3% and 35.6%) in differentiating VT from SVT-A. The Brugada algorithm yielded a sensitivity of 82.2% and specificity of 68.4%. Area under the curve in ROC analysis was highest with Brugada algorithm (0.75, 95% CI 0.69-0.81) followed by QWC-A (0.63, 95% CI 0.56-0.70) and QWC-B (0.59, 95% CI 0.52-0.67).</p><p><strong>Conclusion: </strong>QWC-A and QWC-B criteria had poor sensitivity but high specificity in diagnosing VT in patients presenting with WCT. Further research combining this simple criterion with other newer diagnostic algorithms can potentially improve the accuracy of the overall diagnostic algorithm.</p>\",\"PeriodicalId\":10419,\"journal\":{\"name\":\"Clinical Medicine Insights. Cardiology\",\"volume\":\"14 \",\"pages\":\"1179546820953416\"},\"PeriodicalIF\":3.3000,\"publicationDate\":\"2020-08-30\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://sci-hub-pdf.com/10.1177/1179546820953416\",\"citationCount\":\"2\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Clinical Medicine Insights. Cardiology\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1177/1179546820953416\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2020/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q2\",\"JCRName\":\"CARDIAC & CARDIOVASCULAR SYSTEMS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Clinical Medicine Insights. Cardiology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1177/1179546820953416","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2020/1/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 2
摘要
背景:宽复合心动过速(WCT)与室性心动过速(VT)和室上性心动过速伴畸变(SVT-A)的心电图鉴别常常具有挑战性。目的:比较Brugada算法,探讨下导联(II、III、aVF)中q -波形(QS、Qr、QRs)的存在是否能在WCT中区分VT和SVT-A。我们研究了两个不良导联标准,即QWC-A,所有不良导联都有相似的Q波形,QWC-B只有导联aVF有Q波形。方法:对181例连续WCT病例进行识别,由2名电生理学家进行独立复查,并将其数字化分为心前导联和下导联。根据Brugada和亚导联算法进行VT或SVT-A的心电图诊断。结果与最终临床诊断结果进行比较。结果:24.9%的心电图队列患者(45/181)最终诊断为室性心动过速;75.1%(136/181)为SVT-A。QWC-A和QWC-B鉴别VT与SVT-A的特异性(93.3%、82.8%)和准确性(78.2%、71.0%)较高,敏感性(33.3%、35.6%)较低。Brugada算法的敏感性为82.2%,特异性为68.4%。Brugada算法的ROC分析曲线下面积最高(0.75,95% CI 0.69 ~ 0.81),其次是QWC-A (0.63, 95% CI 0.56 ~ 0.70)和QWC-B (0.59, 95% CI 0.52 ~ 0.67)。结论:QWC-A和QWC-B标准诊断WCT患者室速的敏感性较差,但特异性较高。将这一简单标准与其他较新的诊断算法相结合的进一步研究可能会提高整个诊断算法的准确性。
Utility of Inferior Lead Q-waveforms in diagnosing Ventricular Tachycardia.
Background: Electrocardiogram (ECG) differentiation of wide complex tachycardia (WCT) into ventricular tachycardia (VT) and supraventricular tachycardia with aberration (SVT-A) is often challenging.
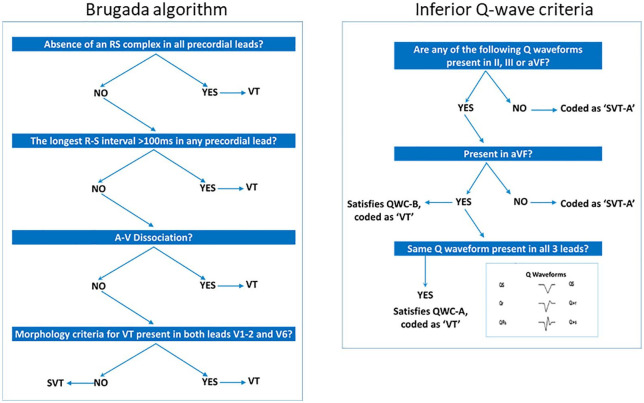
Objective: To determine if the presence of Q-waveforms (QS, Qr, QRs) in the inferior leads (II, III, aVF) can differentiate VT from SVT-A in a WCT compared to Brugada algorithm. We studied 2 inferior lead criteria namely QWC-A where all the inferior leads had a similar Q wave pattern and QWC-B where only lead aVF had a Q-waveform.
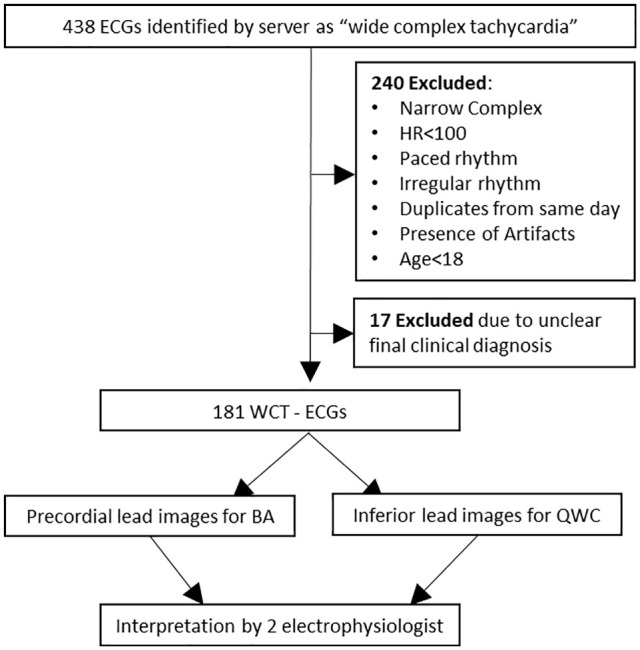
Methods: A total of 181 consecutive cases of WCT were identified, digitally separated into precordial leads and inferior leads and independently reviewed by 2 electrophysiologists. An electrocardiographic diagnosis of VT or SVT-A was assigned based on Brugada and inferior lead algorithms. Results were compared to the final clinical diagnosis.
Results: VT was the final clinical diagnosis in 24.9% of ECG cohort (45/181); 75.1% (136/181) were SVT-A. QWC-A and QWC-B had a high specificity (93.3% and 82.8%) and accuracy (78.2% and 71.0%), but low sensitivity (33.3% and 35.6%) in differentiating VT from SVT-A. The Brugada algorithm yielded a sensitivity of 82.2% and specificity of 68.4%. Area under the curve in ROC analysis was highest with Brugada algorithm (0.75, 95% CI 0.69-0.81) followed by QWC-A (0.63, 95% CI 0.56-0.70) and QWC-B (0.59, 95% CI 0.52-0.67).
Conclusion: QWC-A and QWC-B criteria had poor sensitivity but high specificity in diagnosing VT in patients presenting with WCT. Further research combining this simple criterion with other newer diagnostic algorithms can potentially improve the accuracy of the overall diagnostic algorithm.





 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
