{"title":"JAK2突变阳性骨髓增生性肿瘤伴重度高血压2例","authors":"Raunak Rao, Spoorthy Kulkarni, Ian B Wilkinson","doi":"10.1155/2020/8887423","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Myeloproliferative neoplasms are a heterogeneous group of disorders resulting from the abnormal proliferation of one or more terminal myeloid cells-established complications include thrombosis and haemorrhagic events; however, there is limited evidence to suggest an association with arterial hypertension. Herein, we report two independent cases of severe hypertension in JAK2 mutation-positive myeloproliferative neoplasms. <i>Case Presentations</i>. Case 1: a 39-year-old male was referred to our specialist hypertension unit with high blood pressure (BP) (200/120 mmHg), erythromelalgia, and headaches. We recorded elevated serum creatinine levels (146 <i>μ</i>M) and panmyelosis. Bone marrow biopsy confirmed JAK2-mutation-positive polycythaemia vera. Renal imaging revealed renal artery stenosis. Aspirin, long-acting nifedipine, interferon-alpha 2A, and renal artery angioplasty were employed in management. BP reached below target levels to an average of 119/88 mmHg. Renal parameters normalised gradually alongside BP. Case 2: a 45-year-old male presented with high BP (208/131 mmHg), acrocyanosis, (vasculitic) skin rashes, and nonhealing ulcers. Fundoscopy showed optic disc blurring in the left eye and full blood count revealed thrombocytosis. Bone marrow biopsy confirmed JAK2-mutation-positive essential thrombocytosis. No renal artery stenosis was found. Cardiac output was measured at 5 L/min using an inert gas rebreathing method, providing an estimated peripheral vascular resistance of 1840 dynes/s/cm<sup>5</sup>. BP was well-controlled (reaching 130/70 mmHg) with CCBs.</p><p><strong>Conclusions: </strong>These presentations highlight the utility of full blood count analysis in patients with severe hypertension. Hyperviscosity and constitutive JAK-STAT activation are amongst the proposed pathophysiology linking myeloproliferative neoplasms and hypertension. Further experimental and clinical research is necessary to identify and understand possible interactions between BP and myeloproliferative neoplasms.</p>","PeriodicalId":9632,"journal":{"name":"Case Reports in Vascular Medicine","volume":"2020 ","pages":"8887423"},"PeriodicalIF":0.0000,"publicationDate":"2020-11-09","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.1155/2020/8887423","citationCount":"2","resultStr":"{\"title\":\"Two Cases of Severe Hypertension in JAK2 Mutation-Positive Myeloproliferative Neoplasms.\",\"authors\":\"Raunak Rao, Spoorthy Kulkarni, Ian B Wilkinson\",\"doi\":\"10.1155/2020/8887423\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Myeloproliferative neoplasms are a heterogeneous group of disorders resulting from the abnormal proliferation of one or more terminal myeloid cells-established complications include thrombosis and haemorrhagic events; however, there is limited evidence to suggest an association with arterial hypertension. Herein, we report two independent cases of severe hypertension in JAK2 mutation-positive myeloproliferative neoplasms. <i>Case Presentations</i>. Case 1: a 39-year-old male was referred to our specialist hypertension unit with high blood pressure (BP) (200/120 mmHg), erythromelalgia, and headaches. We recorded elevated serum creatinine levels (146 <i>μ</i>M) and panmyelosis. Bone marrow biopsy confirmed JAK2-mutation-positive polycythaemia vera. Renal imaging revealed renal artery stenosis. Aspirin, long-acting nifedipine, interferon-alpha 2A, and renal artery angioplasty were employed in management. BP reached below target levels to an average of 119/88 mmHg. Renal parameters normalised gradually alongside BP. Case 2: a 45-year-old male presented with high BP (208/131 mmHg), acrocyanosis, (vasculitic) skin rashes, and nonhealing ulcers. Fundoscopy showed optic disc blurring in the left eye and full blood count revealed thrombocytosis. Bone marrow biopsy confirmed JAK2-mutation-positive essential thrombocytosis. No renal artery stenosis was found. Cardiac output was measured at 5 L/min using an inert gas rebreathing method, providing an estimated peripheral vascular resistance of 1840 dynes/s/cm<sup>5</sup>. BP was well-controlled (reaching 130/70 mmHg) with CCBs.</p><p><strong>Conclusions: </strong>These presentations highlight the utility of full blood count analysis in patients with severe hypertension. Hyperviscosity and constitutive JAK-STAT activation are amongst the proposed pathophysiology linking myeloproliferative neoplasms and hypertension. Further experimental and clinical research is necessary to identify and understand possible interactions between BP and myeloproliferative neoplasms.</p>\",\"PeriodicalId\":9632,\"journal\":{\"name\":\"Case Reports in Vascular Medicine\",\"volume\":\"2020 \",\"pages\":\"8887423\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2020-11-09\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://sci-hub-pdf.com/10.1155/2020/8887423\",\"citationCount\":\"2\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Case Reports in Vascular Medicine\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1155/2020/8887423\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2020/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Case Reports in Vascular Medicine","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1155/2020/8887423","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2020/1/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
Two Cases of Severe Hypertension in JAK2 Mutation-Positive Myeloproliferative Neoplasms.
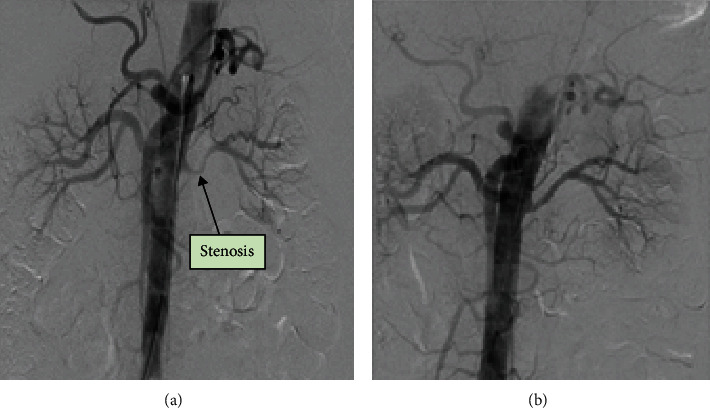
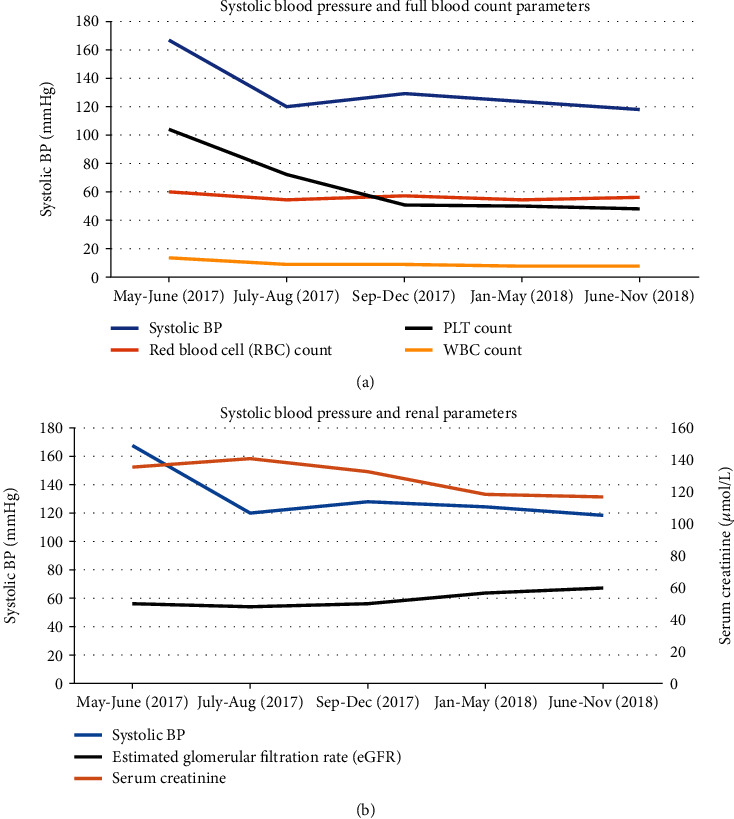
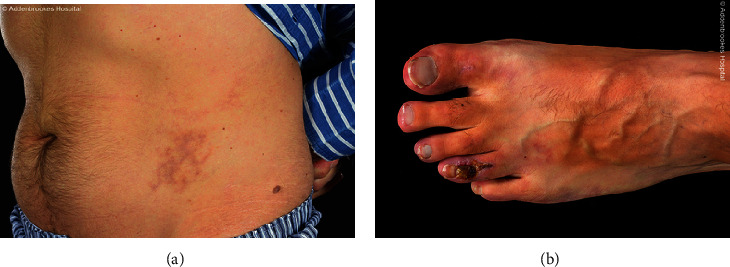
Background: Myeloproliferative neoplasms are a heterogeneous group of disorders resulting from the abnormal proliferation of one or more terminal myeloid cells-established complications include thrombosis and haemorrhagic events; however, there is limited evidence to suggest an association with arterial hypertension. Herein, we report two independent cases of severe hypertension in JAK2 mutation-positive myeloproliferative neoplasms. Case Presentations. Case 1: a 39-year-old male was referred to our specialist hypertension unit with high blood pressure (BP) (200/120 mmHg), erythromelalgia, and headaches. We recorded elevated serum creatinine levels (146 μM) and panmyelosis. Bone marrow biopsy confirmed JAK2-mutation-positive polycythaemia vera. Renal imaging revealed renal artery stenosis. Aspirin, long-acting nifedipine, interferon-alpha 2A, and renal artery angioplasty were employed in management. BP reached below target levels to an average of 119/88 mmHg. Renal parameters normalised gradually alongside BP. Case 2: a 45-year-old male presented with high BP (208/131 mmHg), acrocyanosis, (vasculitic) skin rashes, and nonhealing ulcers. Fundoscopy showed optic disc blurring in the left eye and full blood count revealed thrombocytosis. Bone marrow biopsy confirmed JAK2-mutation-positive essential thrombocytosis. No renal artery stenosis was found. Cardiac output was measured at 5 L/min using an inert gas rebreathing method, providing an estimated peripheral vascular resistance of 1840 dynes/s/cm5. BP was well-controlled (reaching 130/70 mmHg) with CCBs.
Conclusions: These presentations highlight the utility of full blood count analysis in patients with severe hypertension. Hyperviscosity and constitutive JAK-STAT activation are amongst the proposed pathophysiology linking myeloproliferative neoplasms and hypertension. Further experimental and clinical research is necessary to identify and understand possible interactions between BP and myeloproliferative neoplasms.



 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
